You might also like
- Bio ProjectDocument19 pagesBio Projectsamarthmathur014No ratings yet
- guidelines-for-diagnosis2011Document22 pagesguidelines-for-diagnosis2011Soumalya GhoshNo ratings yet
- Treatment of Malaria (Guidelines For Clinicians)Document8 pagesTreatment of Malaria (Guidelines For Clinicians)Razvan RzNo ratings yet
- Malaria Diagnosis Methods Brief ReviewDocument10 pagesMalaria Diagnosis Methods Brief ReviewFir FurqaniNo ratings yet
- Malaria TRX Guide For US Clinicians 202302cDocument8 pagesMalaria TRX Guide For US Clinicians 202302cDanuNo ratings yet
- Clinicalguidance Malaria Treatment, CDCDocument8 pagesClinicalguidance Malaria Treatment, CDCSultanaNo ratings yet
- Diagnosi S: MalariaDocument28 pagesDiagnosi S: MalariaOm Prakash SinghNo ratings yet
- Evaluationa Vivaks LembataDocument10 pagesEvaluationa Vivaks Lembatamichael biaNo ratings yet
- Management of MalariaDocument39 pagesManagement of MalariaDileep SableNo ratings yet
- Malaria ProjectDocument45 pagesMalaria ProjectNikhilNo ratings yet
- Malaria Case AnalysisDocument1 pageMalaria Case AnalysisANGELA MARIE VILLENANo ratings yet
- The Management of Patients With Severe Malaria: AbstractDocument7 pagesThe Management of Patients With Severe Malaria: AbstractHervi LaksariNo ratings yet
- Drug Policy 08Document13 pagesDrug Policy 08egalivanNo ratings yet
- National Maria Drug Policy 2007Document12 pagesNational Maria Drug Policy 2007drbeerappa janpetNo ratings yet
- Diagnosis of MalariaDocument15 pagesDiagnosis of MalariaSuranjan Pal100% (1)
- Managing Severe Malaria CasesDocument100 pagesManaging Severe Malaria CasesAshis karmakarNo ratings yet
- Guidlines For MalariaDocument10 pagesGuidlines For MalariaObitracks SarahadilNo ratings yet
- Malaria 1. Who and How?: P. Falciparum P. VivaxDocument6 pagesMalaria 1. Who and How?: P. Falciparum P. VivaxAdriana del RioNo ratings yet
- Consultant Physician, NDUTH: MBBS, FWACP, FMCP-Infectious DiseaseDocument46 pagesConsultant Physician, NDUTH: MBBS, FWACP, FMCP-Infectious DiseasePrincewill SeiyefaNo ratings yet
- Current Trends in The Management of MalariaDocument41 pagesCurrent Trends in The Management of Malariaghr9cjy5npNo ratings yet
- Malaria: Michael Aguilar, RMTDocument27 pagesMalaria: Michael Aguilar, RMTFrankenstein MelancholyNo ratings yet
- Malaria Treatment Guidelines-2 ND Edition 2011Document210 pagesMalaria Treatment Guidelines-2 ND Edition 2011Kevins KhaembaNo ratings yet
- Malaria Treatment Guidelines WHO 2010Document211 pagesMalaria Treatment Guidelines WHO 2010emc27No ratings yet
- Pediatric Malaria Treatment & Management: Approach Considerations, Intensive Care, Deterrence and PreventionDocument4 pagesPediatric Malaria Treatment & Management: Approach Considerations, Intensive Care, Deterrence and PreventionVivi DeviyanaNo ratings yet
- Notes On NHP - MalariaDocument6 pagesNotes On NHP - MalariaViswa GiriNo ratings yet
- MalariaDocument72 pagesMalariajvNo ratings yet
- National Antimalarial Drug Policy for YemenDocument19 pagesNational Antimalarial Drug Policy for YemenAmmarNo ratings yet
- Guidelines Malaria Di MalaysiaDocument61 pagesGuidelines Malaria Di MalaysianalmifaNo ratings yet
- Malaria PreventionDocument35 pagesMalaria PreventionRaúlNo ratings yet
- Diagnosis Treatment MalariaDocument29 pagesDiagnosis Treatment MalariaAnuradha Akolekar-mahadik100% (1)
- Malaria MettyDocument13 pagesMalaria MettySiti Qomariah AnisaNo ratings yet
- MalariaDocument3 pagesMalariaGuna SoundariNo ratings yet
- Malaria: Nama: Rismawati NIM: C 111 09 752Document6 pagesMalaria: Nama: Rismawati NIM: C 111 09 752Rismawati AcenkNo ratings yet
- Treatment of Malaria-Guidelines For Clinicians WHO PDFDocument9 pagesTreatment of Malaria-Guidelines For Clinicians WHO PDFMuhammad Arman ArraufNo ratings yet
- National Antimalarial Drug Policy - YemenDocument17 pagesNational Antimalarial Drug Policy - YemenAmmarNo ratings yet
- Malaria in PregnancyDocument28 pagesMalaria in PregnancyPeprah Ondiba100% (1)
- Mosquito-borne Malaria DiseaseDocument12 pagesMosquito-borne Malaria Diseasespiderind2No ratings yet
- Peace Client Care WorkDocument29 pagesPeace Client Care WorkVANGAWA JOHNNo ratings yet
- WHO - MalariaDocument7 pagesWHO - Malariareborn007No ratings yet
- Examination Card 10Document9 pagesExamination Card 10FUTURE DOCTORNo ratings yet
- 8 Malaria Is An Uncommon Cause of Adult Sepsis in SouthDocument9 pages8 Malaria Is An Uncommon Cause of Adult Sepsis in SouthAhmad Zaki YamaniNo ratings yet
- Insecticide ResistanceDocument3 pagesInsecticide ResistanceGenniNo ratings yet
- Web-Based Healthcare For MalariaDocument3 pagesWeb-Based Healthcare For MalariaOffice OpenNo ratings yet
- Malaria DiseaseDocument33 pagesMalaria DiseaseSteni TriscaNo ratings yet
- NPMCN Update Course 2011 Malaria TherapyDocument69 pagesNPMCN Update Course 2011 Malaria TherapyIsmail RajiNo ratings yet
- Eng FullDocument266 pagesEng FullHervi LaksariNo ratings yet
- Epidemiology & Control of Tropical DiseaseDocument38 pagesEpidemiology & Control of Tropical DiseaseMazinNo ratings yet
- Green Top Guidelines 13Document29 pagesGreen Top Guidelines 13garfield1No ratings yet
- Malaria Pregnancy RcogDocument29 pagesMalaria Pregnancy RcogBonifacius Bayu Erlangga KusumaNo ratings yet
- Role of ACT, S & WHO Guidlines For The Treatment of MalariaDocument34 pagesRole of ACT, S & WHO Guidlines For The Treatment of MalariasalmanNo ratings yet
- Malaria: What's New in The Management of Malaria?Document22 pagesMalaria: What's New in The Management of Malaria?wiwiNo ratings yet
- Management - Guidelines - of - Malaria - in - Malaysia - (Final) v2 PDFDocument63 pagesManagement - Guidelines - of - Malaria - in - Malaysia - (Final) v2 PDFaiyuanNo ratings yet
- Malaria in NigeriaDocument1 pageMalaria in Nigeriaahmad hauwauNo ratings yet
- Artesunate for Severe MalariaDocument9 pagesArtesunate for Severe Malariabaitur_rohmah8372No ratings yet
- Clinically Relevant Mycoses: A Practical ApproachFrom EverandClinically Relevant Mycoses: A Practical ApproachElisabeth PresterlNo ratings yet
- Integrated Disease Surveillance and Response (IDSR) in AfricaFrom EverandIntegrated Disease Surveillance and Response (IDSR) in AfricaRating: 5 out of 5 stars5/5 (1)
- Malaria: A Comprehensive Guide to Symptoms, Self-Care, Diet Plans, Herbal and Homeopathic Remedies: Homeopathy, #1From EverandMalaria: A Comprehensive Guide to Symptoms, Self-Care, Diet Plans, Herbal and Homeopathic Remedies: Homeopathy, #1No ratings yet
- Health Guidelines For Schools Reopening During COVID 19 Pandemic - 3601v5 AH2 AMA (21343)Document17 pagesHealth Guidelines For Schools Reopening During COVID 19 Pandemic - 3601v5 AH2 AMA (21343)jamshaidjiNo ratings yet
- VPD Surveillance Guidelines - PunjabDocument91 pagesVPD Surveillance Guidelines - PunjabjamshaidjiNo ratings yet
- WHO Key Facts Nipah Virus InfectionDocument6 pagesWHO Key Facts Nipah Virus InfectionjamshaidjiNo ratings yet
- Malaysia c19 Case Study 20 AugustDocument9 pagesMalaysia c19 Case Study 20 AugustHaliza MdesaNo ratings yet
- Who Nipah Baseline Situation Analysis 27jan2018Document41 pagesWho Nipah Baseline Situation Analysis 27jan2018jamshaidjiNo ratings yet
- WHO 2019 nCoV Ramadan 2020.1 EngDocument3 pagesWHO 2019 nCoV Ramadan 2020.1 EngManami OkuNo ratings yet
- EMRO Core IndicatorsDocument1 pageEMRO Core IndicatorsjamshaidjiNo ratings yet
- Checklist For Assessment of Outpatient Services in Hospitals in Context of COVID-19Document2 pagesChecklist For Assessment of Outpatient Services in Hospitals in Context of COVID-19jamshaidji0% (1)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Emropub 2016 en 19266Document45 pagesEmropub 2016 en 19266jamshaidjiNo ratings yet
- Emropub 2015 en 1887Document18 pagesEmropub 2015 en 1887jamshaidjiNo ratings yet
- Module 2 Natural History and Clinical AspectsDocument38 pagesModule 2 Natural History and Clinical AspectsDrMansoor MemonNo ratings yet
- WHO Key Facts Nipah Virus InfectionDocument6 pagesWHO Key Facts Nipah Virus InfectionjamshaidjiNo ratings yet
- WHO Key Facts Nipah Virus InfectionDocument6 pagesWHO Key Facts Nipah Virus InfectionjamshaidjiNo ratings yet
- HIV Testing: DR Quaid SaeedDocument21 pagesHIV Testing: DR Quaid SaeedjamshaidjiNo ratings yet
- Campaign Monitoring PlanDocument3 pagesCampaign Monitoring PlanjamshaidjiNo ratings yet
- Pakistan: National Youth Shadow ReportDocument13 pagesPakistan: National Youth Shadow ReportjamshaidjiNo ratings yet
- Uncomplicated Malaria: Malaria: Standard Case Definitions: Suspected CaseDocument4 pagesUncomplicated Malaria: Malaria: Standard Case Definitions: Suspected CasejamshaidjiNo ratings yet
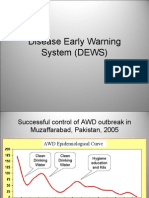
- DEWSDocument31 pagesDEWSjamshaidjiNo ratings yet
- Full Page PhotoDocument1 pageFull Page PhotojamshaidjiNo ratings yet
- List of Pharmaceutical Companies in PuneDocument5 pagesList of Pharmaceutical Companies in PuneMain Sanatani HunNo ratings yet
- Caffeine: The Good, The Bad, and The UglyDocument4 pagesCaffeine: The Good, The Bad, and The UglyBerenice RomeroNo ratings yet
- The Thalidomide HistoryDocument11 pagesThe Thalidomide HistoryJesus VuelvasNo ratings yet
- Hospital Case StudyDocument7 pagesHospital Case StudyEfrén Pérez BernabeNo ratings yet
- ECA CrossContamination PDFDocument4 pagesECA CrossContamination PDFtamiNo ratings yet
- Hair Analysis For The Detection of Drug Use - Is There Potential For EvasionDocument7 pagesHair Analysis For The Detection of Drug Use - Is There Potential For EvasionTymon BlaksellNo ratings yet
- Antimicrobial Activity and Resistance: Influencing FactorsDocument11 pagesAntimicrobial Activity and Resistance: Influencing FactorsKamila HidalgoNo ratings yet
- Introduction To Drug Discovery and DevelopmentDocument25 pagesIntroduction To Drug Discovery and Developmentafnanosman2002No ratings yet
- CV Health Management ConsultantDocument2 pagesCV Health Management ConsultantApriansyahNo ratings yet
- Toppers List 2010Document2 pagesToppers List 2010Sri Krishna ChaithanyaNo ratings yet
- Non Linear PharmacokineticsDocument33 pagesNon Linear PharmacokineticsClaudNo ratings yet
- Paediatric Doses of DrugsDocument2 pagesPaediatric Doses of DrugsumapathisivanNo ratings yet
- ZegenDocument9 pagesZegenJefferson ManasanNo ratings yet
- Pharmacology Bundle Study GuideDocument47 pagesPharmacology Bundle Study GuideAmisalu NigusieNo ratings yet
- In DirectorsDocument200 pagesIn DirectorsRavindra T MakunteNo ratings yet
- Product Lifecycle in Pharmaceutical Industry Journey of Drug From Ideation To CommercializationDocument13 pagesProduct Lifecycle in Pharmaceutical Industry Journey of Drug From Ideation To CommercializationAmit ChoudharyNo ratings yet
- 24 Ilukor 279289Document56 pages24 Ilukor 279289Masood AalamNo ratings yet
- Raise Your Game Expand Your Horizons in The Indian OTC MarketDocument5 pagesRaise Your Game Expand Your Horizons in The Indian OTC MarketAnkit DalmiaNo ratings yet
- Medical Devices Industry and Market Propects 2013-2023 PDFDocument21 pagesMedical Devices Industry and Market Propects 2013-2023 PDFVisiongainGlobal33% (3)
- Dissolution and Drug Release TestingDocument20 pagesDissolution and Drug Release TestingfisesaNo ratings yet
- VP Sales Biotech Pharmaceuticals in Atlanta GA Resume Valerie DarlingDocument2 pagesVP Sales Biotech Pharmaceuticals in Atlanta GA Resume Valerie DarlingValerieDarlingNo ratings yet
- Jock ItchDocument16 pagesJock ItchMarcz Leogan BriagasNo ratings yet
- Kohlberg's Theory of Moral Development and the Heinz DilemmaDocument18 pagesKohlberg's Theory of Moral Development and the Heinz DilemmaCassy Pontemayor100% (1)
- Hydroxychloroquine SulfateDocument20 pagesHydroxychloroquine Sulfategiamatti2005No ratings yet
- Metoclopramide for GERD and gastroparesisDocument5 pagesMetoclopramide for GERD and gastroparesisHana HanaNo ratings yet
- AdrDocument9 pagesAdrvizzladNo ratings yet
- AmbrolexDocument4 pagesAmbrolexWeiki Opan FirdausNo ratings yet
- Math Practice For Paramedic StudentsDocument8 pagesMath Practice For Paramedic StudentsGreg Zeitlin50% (2)
- Antihistamine - WikipediaDocument39 pagesAntihistamine - WikipediaMuhammadafif SholehuddinNo ratings yet