You might also like
- Ssti PDFDocument4 pagesSsti PDFflori.bNo ratings yet
- WHO Definition of Palliative CareDocument6 pagesWHO Definition of Palliative CareDefri RahmanNo ratings yet
- Surat Insip Feb 2014 UndipDocument1 pageSurat Insip Feb 2014 UndipRisma J AsifNo ratings yet
- Hepatitis C, Hirlan Dan Hery Overview DR - HirlanDocument28 pagesHepatitis C, Hirlan Dan Hery Overview DR - HirlanRisma J AsifNo ratings yet
- Graduate School Scholarship Programme InfoDocument1 pageGraduate School Scholarship Programme InfoRisma J AsifNo ratings yet
- DR Villy Muscle RelaxantDocument22 pagesDR Villy Muscle RelaxantRisma J AsifNo ratings yet
- Weel CriteriaDocument6 pagesWeel CriteriaRisma J AsifNo ratings yet
- Dengue AdvisoryDocument9 pagesDengue AdvisoryLlean Jessica DeVega TanNo ratings yet
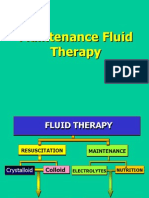
- Maintenance - Fluid-Bahan Matrikulasi Penyakit DalamDocument27 pagesMaintenance - Fluid-Bahan Matrikulasi Penyakit DalamRisma J AsifNo ratings yet
- Trauma KimiaDocument7 pagesTrauma KimiaRisma J AsifNo ratings yet
- Membrane, Electrolyte and Water BalanceDocument26 pagesMembrane, Electrolyte and Water BalanceRisma J AsifNo ratings yet
- Dengue Vaccines Approach The Finish Line: SupplementarticleDocument5 pagesDengue Vaccines Approach The Finish Line: SupplementarticleRisma J AsifNo ratings yet
- Logo UndipDocument1 pageLogo UndipRisma J AsifNo ratings yet
- Logo UndipDocument1 pageLogo UndipRisma J AsifNo ratings yet
- Lepto ChennaiDocument17 pagesLepto ChennaiRisma J AsifNo ratings yet
- Logo UndipDocument1 pageLogo UndipRisma J AsifNo ratings yet
- Hipertensi EmergensiDocument37 pagesHipertensi EmergensiRisma J AsifNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Lecture Notes - MobilityDocument9 pagesLecture Notes - MobilityAileen DonahueNo ratings yet
- Articulo Asma Felina 1 PDFDocument5 pagesArticulo Asma Felina 1 PDFTania GonzalezNo ratings yet
- ASSESSMENT OF THE EAR, NOSE, MOUTH AND THROAT (Chapter 12)Document4 pagesASSESSMENT OF THE EAR, NOSE, MOUTH AND THROAT (Chapter 12)Christianne CapuaNo ratings yet
- Blood Glucose: Hemoatocrit (%) / Hemoglobin (G/DL)Document4 pagesBlood Glucose: Hemoatocrit (%) / Hemoglobin (G/DL)Stacy ChoiNo ratings yet
- Clincal Case Presentation 5Document32 pagesClincal Case Presentation 5api-635948254No ratings yet
- ICMM Health and Safety Performance Indicator DefinitionsDocument34 pagesICMM Health and Safety Performance Indicator DefinitionsStakeholders360No ratings yet
- Respiratory System: Copd (Bronchitis & Emphysema)Document7 pagesRespiratory System: Copd (Bronchitis & Emphysema)Rhea Lyn LamosteNo ratings yet
- Case Study For Respiratory SystemDocument3 pagesCase Study For Respiratory System︻╦̵̵͇̿̿̿̿╤── Rico Zaemowrah100% (2)
- Internal MedicineDocument117 pagesInternal MedicineRichard MelialaNo ratings yet
- Medical Revision PaperDocument106 pagesMedical Revision PaperDavin SugumarNo ratings yet
- Asthma Clinical Care GuidelinesDocument17 pagesAsthma Clinical Care GuidelinesWalaa MoustafaNo ratings yet
- Comparison of Artificial Intelligence Versus Real Time PhysicianDocument4 pagesComparison of Artificial Intelligence Versus Real Time PhysicianYony GutierrezNo ratings yet
- Aling Juana, 42 Years Old, FemaleDocument2 pagesAling Juana, 42 Years Old, FemaleGenynne RagasaNo ratings yet
- A Group of Homoeopathic Medicines For COVID 19: A Systematic Review of Clinical FeaturesDocument18 pagesA Group of Homoeopathic Medicines For COVID 19: A Systematic Review of Clinical FeaturesY.rajuNo ratings yet
- 10th Ecc Uk Annual Congress Course Notes 2013 PDFDocument334 pages10th Ecc Uk Annual Congress Course Notes 2013 PDFdwiNo ratings yet
- Palliative Care Tools - Technical Brief 2017 PDFDocument145 pagesPalliative Care Tools - Technical Brief 2017 PDFMas AnggaNo ratings yet
- Indian Journal of Physiotherapy and Occupational TherapyDocument8 pagesIndian Journal of Physiotherapy and Occupational TherapygulbudNo ratings yet
- Chest PainDocument3 pagesChest Painkhairiah09No ratings yet
- BPUDDocument26 pagesBPUDIvanNo ratings yet
- HTN Urgency Case StudyDocument4 pagesHTN Urgency Case StudyJavin TNo ratings yet
- FAELDONEA, PJ - Nursing Care PlanDocument6 pagesFAELDONEA, PJ - Nursing Care PlanPatricia Jean Faeldonea100% (1)
- CHIEF COMPLAINTS: - Difficulty of BreathingDocument61 pagesCHIEF COMPLAINTS: - Difficulty of BreathingjonelloveuvarnalNo ratings yet
- Disorders of The Respiratory SystemDocument9 pagesDisorders of The Respiratory SystemAjay Pal NattNo ratings yet
- Post Test 02Document3 pagesPost Test 02Evangeline Olarte QuilantangNo ratings yet
- Dyspnea Review For The Palliative Care Professional Treatment Goals and Therapeutic OptionsDocument10 pagesDyspnea Review For The Palliative Care Professional Treatment Goals and Therapeutic OptionsAndres SiwiNo ratings yet
- NPDADocument52 pagesNPDAAlondra MangandogNo ratings yet
- Bronchial Asthma (Case Study)Document12 pagesBronchial Asthma (Case Study)Adriane Coma100% (1)
- PTB NCPDocument12 pagesPTB NCPNiel LeeNo ratings yet
- Medical Report - Ayu DyahDocument7 pagesMedical Report - Ayu DyahKusumadewi WidiarsaNo ratings yet
- Lung Meridian PDFDocument1 pageLung Meridian PDFrinkyNo ratings yet