You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- PeripheralDocument25 pagesPeripheralMans FansNo ratings yet
- AnemiaDocument88 pagesAnemiaMans FansNo ratings yet
- DR: Abd El Hameed Fureeh: MD, Lecturer of Internal Medicine, Mansoura Faculty of MedicineDocument91 pagesDR: Abd El Hameed Fureeh: MD, Lecturer of Internal Medicine, Mansoura Faculty of MedicineMans Fans100% (2)
- Typhoid Fever: (Enterica)Document22 pagesTyphoid Fever: (Enterica)Mans FansNo ratings yet
- LymphomaDocument40 pagesLymphomaMans Fans100% (1)
- Glomerulonephritis 2Document56 pagesGlomerulonephritis 2Mans FansNo ratings yet
- Curriculum Vittae Curriculum Vittae Curriculum Vittae: Dr. Mahmoud El-WasifyDocument16 pagesCurriculum Vittae Curriculum Vittae Curriculum Vittae: Dr. Mahmoud El-WasifyMans Fans100% (1)
- Polycythemia.mansfans.comDocument14 pagesPolycythemia.mansfans.comMans FansNo ratings yet
- Anxiety Disorders: Wafaa El-BahaeyDocument41 pagesAnxiety Disorders: Wafaa El-BahaeyMans FansNo ratings yet
- Teratogenic Agents and TheirDocument23 pagesTeratogenic Agents and TheirMans Fans100% (2)
- Copd UpdateDocument65 pagesCopd UpdateMans FansNo ratings yet
- Prof. Mohammad Khairy.... Symptoms & Signs of Chest DiseasesDocument121 pagesProf. Mohammad Khairy.... Symptoms & Signs of Chest DiseasesMans FansNo ratings yet
- DR - Mohamed Awad Lect. Medical Oncology CMU MD, NCI, Cairo UniversityDocument21 pagesDR - Mohamed Awad Lect. Medical Oncology CMU MD, NCI, Cairo UniversityMans FansNo ratings yet
- Tumor Markers Some Laboratory Aspects of Pregnancy Cerebrospinal Fluid AnalysisDocument40 pagesTumor Markers Some Laboratory Aspects of Pregnancy Cerebrospinal Fluid AnalysisMans FansNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- NABH Series2 COPDocument63 pagesNABH Series2 COPPallavi Deepak DongreNo ratings yet
- Intervertebral Disc ProlapseDocument18 pagesIntervertebral Disc Prolapsemeto67% (3)
- Algoritmo de La Gasometría ArterialDocument15 pagesAlgoritmo de La Gasometría ArterialJhonatan Efraín López CarbajalNo ratings yet
- Daftar PustakaDocument8 pagesDaftar PustakaErmaffNo ratings yet
- Drug StudyDocument5 pagesDrug StudySarie LevitaNo ratings yet
- PhysiologyDocument31 pagesPhysiologyraza20100% (1)
- 62 Lecture Menstrual Cycle Abnormalities, Infertility, MenopauseDocument69 pages62 Lecture Menstrual Cycle Abnormalities, Infertility, MenopauseTarek TarekNo ratings yet
- Cashless Authorisation Requisition FormDocument1 pageCashless Authorisation Requisition FormPandurangaNo ratings yet
- English Task - Multiple Choices - 20200102Document8 pagesEnglish Task - Multiple Choices - 20200102bangtan's elite trashNo ratings yet
- 100 MCQs-3Document19 pages100 MCQs-3hassan qureshiNo ratings yet
- Wellness CenterDocument6 pagesWellness CenterMuntasir SizanNo ratings yet
- Epifix Amniofix InformationDocument11 pagesEpifix Amniofix Informationapi-235072265100% (1)
- Master of Science in RadiodiagnosisDocument73 pagesMaster of Science in RadiodiagnosisCwali MohamedNo ratings yet
- Critical Care NursingDocument5 pagesCritical Care NursingMK BelitungNo ratings yet
- The Journey of Antibody and Antigen Test During COVID-19 Pandemic in Indonesia, The Advantages & DisadvantagesDocument34 pagesThe Journey of Antibody and Antigen Test During COVID-19 Pandemic in Indonesia, The Advantages & DisadvantagesEldo TaufilaNo ratings yet
- Mnemonics Psychiatric Diagnosis.Document7 pagesMnemonics Psychiatric Diagnosis.عمر الحدادNo ratings yet
- Cholangitis and Cholecystitis (DR - Dr. Hery Djagat Purnomo, SpPD-KGEH)Document47 pagesCholangitis and Cholecystitis (DR - Dr. Hery Djagat Purnomo, SpPD-KGEH)Aditya SahidNo ratings yet
- Assessment: Facial ShavingDocument2 pagesAssessment: Facial ShavingA CNo ratings yet
- Chapter 15 - Dental CariesDocument23 pagesChapter 15 - Dental CariesShoyo HinataNo ratings yet
- Tooth Preparations Science & Art PDFDocument315 pagesTooth Preparations Science & Art PDFИгорь Сидоренко50% (2)
- Cognitive Behavioural Therapy For ADHD in Adults Systematic ReviewDocument9 pagesCognitive Behavioural Therapy For ADHD in Adults Systematic ReviewDana Ben SimonNo ratings yet
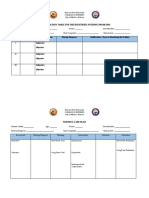
- Prioritization Table For The Identified Nursing ProblemsDocument3 pagesPrioritization Table For The Identified Nursing ProblemsMia PascualNo ratings yet
- I Want My MummyDocument8 pagesI Want My MummyPaulaNo ratings yet
- Circulatory System - Babli YadavDocument13 pagesCirculatory System - Babli YadavBabli YadavNo ratings yet
- Presentation 5 Hand HygieneDocument26 pagesPresentation 5 Hand HygieneAfeefa Amin AliNo ratings yet
- Cleveland Clinic Facts and FiguresDocument2 pagesCleveland Clinic Facts and FiguresUzair Ul GhaniNo ratings yet
- Cesarean BirthDocument35 pagesCesarean BirthJhonny Paul RamosNo ratings yet
- Adult Hip (2nd Edition)Document1,693 pagesAdult Hip (2nd Edition)Jocelyne SturridgeNo ratings yet
- Origin of HIVDocument18 pagesOrigin of HIVRobert SineNo ratings yet
- CP100MEDICALtermPSAbbr. 2Document78 pagesCP100MEDICALtermPSAbbr. 2RAISA N. RASIDNo ratings yet