You might also like
- Sources of PowerDocument1 pageSources of PowerFrench Pastolero-ManaloNo ratings yet
- Thinking Outside The Box CaseDocument3 pagesThinking Outside The Box CaseTan Novinna56% (9)
- Post-Positivist Approaches To ResearchDocument15 pagesPost-Positivist Approaches To Researchmohdii_79100% (1)
- Ethics in Psychological ResearchDocument2 pagesEthics in Psychological ResearchJhunitz LopezNo ratings yet
- Culture Bound Syndrome-3Document55 pagesCulture Bound Syndrome-3pavan kumarNo ratings yet
- Introduction To Psychology: Case Study MethodDocument10 pagesIntroduction To Psychology: Case Study MethodUkhadi 2525No ratings yet
- Industrial Psychology Module 2022 ZANEDocument58 pagesIndustrial Psychology Module 2022 ZANEKeanna Mae DumaplinNo ratings yet
- Cabadbaran City Sanggunian ResolutionDocument2 pagesCabadbaran City Sanggunian ResolutionAlbert CongNo ratings yet
- Notes in Purposive BehaviorismDocument1 pageNotes in Purposive Behaviorismadrienne kaye balazaNo ratings yet
- Psychological TestingDocument15 pagesPsychological TestingAllysa Marie BorladoNo ratings yet
- Module One ChaPTER ONE - PsychDocument15 pagesModule One ChaPTER ONE - PsychArvella Albay100% (1)
- Intelligence and Its Measures 2Document44 pagesIntelligence and Its Measures 2Vincent Rafael AbeciaNo ratings yet
- PDFDocument827 pagesPDFPrince SanjuNo ratings yet
- Positioning & DrapingDocument27 pagesPositioning & DrapingJennifer Solano Cruel100% (5)
- Positioning & DrapingDocument27 pagesPositioning & DrapingJennifer Solano Cruel100% (5)
- Theory of Planned Behavior - WikipediaDocument9 pagesTheory of Planned Behavior - Wikipediawaqas331100% (1)
- EthicsPr VulnerableDocument38 pagesEthicsPr VulnerableTeresa LeachNo ratings yet
- Mixed Methods Research in SchoDocument19 pagesMixed Methods Research in Schooperas69No ratings yet
- Social Psychology NotesDocument64 pagesSocial Psychology Notesfathima1991No ratings yet
- Health Belief ModelDocument3 pagesHealth Belief ModelPrem Deep100% (1)
- Abnormal EssayDocument2 pagesAbnormal EssayBamNo ratings yet
- TCS-SASTRA MCA Program FAQDocument7 pagesTCS-SASTRA MCA Program FAQmanikanta tarunNo ratings yet
- Manual de Genetica Medica (2007)Document519 pagesManual de Genetica Medica (2007)Mara PitrezNo ratings yet
- Belmont CITIDocument9 pagesBelmont CITIaw1435100% (1)
- Pajares y Valiente 2002 Student S Self Efficacy in Their Self Regulated Learning StrategiesDocument11 pagesPajares y Valiente 2002 Student S Self Efficacy in Their Self Regulated Learning StrategiesJuan Hernández García100% (1)
- 17 Health Behavioral ModelsDocument49 pages17 Health Behavioral ModelsVesley B Robin100% (2)
- Lit Review Resilience TheoryDocument27 pagesLit Review Resilience TheoryAnthony Solina100% (3)
- Health Belief Model - Behavioural ChangeDocument3 pagesHealth Belief Model - Behavioural ChangenieotyagiNo ratings yet
- Health Belief ModelDocument6 pagesHealth Belief ModelKesha Hammond100% (1)
- Chapter 1, Introduction To Health PsychologyDocument34 pagesChapter 1, Introduction To Health PsychologyHalimaNo ratings yet
- Assignment Submitted by 1001004: Definitions of PersonalityDocument13 pagesAssignment Submitted by 1001004: Definitions of PersonalitySumaiya SarwatNo ratings yet
- George KellyDocument21 pagesGeorge KellyIly IsaNo ratings yet
- How The Experimental Method Works in Psychology-1Document55 pagesHow The Experimental Method Works in Psychology-1Paul MorakinyoNo ratings yet
- Chapter 5 Personality and Values What Is Personality Defining PersonalityDocument3 pagesChapter 5 Personality and Values What Is Personality Defining PersonalityHannah Go100% (1)
- Chapter 3 - Research MethodologiesDocument28 pagesChapter 3 - Research MethodologiesFarizal ResatNo ratings yet
- Abpc1203 Psychological Tests and MeasurementsDocument14 pagesAbpc1203 Psychological Tests and MeasurementsSiva100% (1)
- Aggression Evolutionary PSYA3Document16 pagesAggression Evolutionary PSYA3careyallenNo ratings yet
- Answers and References 3 1Document32 pagesAnswers and References 3 1Cla RisseNo ratings yet
- EBP Tutorial Intro Critical Appraisal SkillsDocument11 pagesEBP Tutorial Intro Critical Appraisal Skillsbabah79No ratings yet
- Critical ParadigmDocument8 pagesCritical ParadigmramonaNo ratings yet
- Characteristics of Stressful EventsDocument4 pagesCharacteristics of Stressful EventsDamnum Absque InjuriaNo ratings yet
- Chapter 3 Psycho Metrics Reliatility ValidityDocument23 pagesChapter 3 Psycho Metrics Reliatility ValidityUzaima SiddiquiNo ratings yet
- Research ProposalDocument4 pagesResearch ProposalAmmara Aman100% (1)
- Impression Formation & Management/SOCIAL PERCEPTIONDocument9 pagesImpression Formation & Management/SOCIAL PERCEPTIONPrateek KhandelwalNo ratings yet
- Contemporary PsychologyDocument4 pagesContemporary PsychologyZunair IlyasNo ratings yet
- 4.1 Social InteractionDocument20 pages4.1 Social Interactionsabahat saeed100% (1)
- Health Promotion ModelDocument3 pagesHealth Promotion ModelJehannah Dayanara Berdan HayudiniNo ratings yet
- SynopsisDocument3 pagesSynopsisRajalakshmiNo ratings yet
- From Anxiety To Positivity Prevalence and Associated Factors of Anxiety Among Newly Graduated StudentsDocument20 pagesFrom Anxiety To Positivity Prevalence and Associated Factors of Anxiety Among Newly Graduated StudentsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- ValidityDocument16 pagesValidityNinasakinah Mp ArzNo ratings yet
- Descriptive Research: Characteristics Value, Importance, and Advantages TechniquesDocument9 pagesDescriptive Research: Characteristics Value, Importance, and Advantages TechniquesApril MataloteNo ratings yet
- Personality Psychologist Are More Likely To Attribute Errant Behavior To A Person's Enduring TraitsDocument17 pagesPersonality Psychologist Are More Likely To Attribute Errant Behavior To A Person's Enduring TraitsMARIE ROSE L. FUNTANARNo ratings yet
- Methods of PsychologyDocument24 pagesMethods of PsychologyFathima NoreenNo ratings yet
- Statistical TestsDocument15 pagesStatistical Testscharlene quiambaoNo ratings yet
- Attribution TheoryDocument4 pagesAttribution TheoryShanmuga VadivuNo ratings yet
- Nelson & Quick: Personality, Perception, and AttributionDocument22 pagesNelson & Quick: Personality, Perception, and AttributionqberbawroNo ratings yet
- Theories of AggressionDocument4 pagesTheories of AggressionJael100% (1)
- Chapter - Iii Research MethodolgyDocument3 pagesChapter - Iii Research MethodolgyPrince Carl MolinaNo ratings yet
- Imitation of Film-Mediated Aggressive ModelsDocument9 pagesImitation of Film-Mediated Aggressive Modelsoortiz10No ratings yet
- Midterm Study Notes Psy1101Document16 pagesMidterm Study Notes Psy1101Simon HagosNo ratings yet
- Whatis Critical AppraisalDocument8 pagesWhatis Critical Appraisalapi-3861522No ratings yet
- Bystander Intervention EssayDocument9 pagesBystander Intervention EssayAmanda100% (1)
- Humanistic Theory of Learning-Wps OfficeDocument11 pagesHumanistic Theory of Learning-Wps OfficePriscilla KiemoNo ratings yet
- Statistics-: Data Is A Collection of FactsDocument3 pagesStatistics-: Data Is A Collection of FactsLonnieAllenVirtudesNo ratings yet
- Factors Affecting Healthy BehavioursDocument5 pagesFactors Affecting Healthy BehavioursMeghna GaneshNo ratings yet
- Lay ModelDocument17 pagesLay ModelNoor ShahzadNo ratings yet
- Health Belief Model HandoutDocument2 pagesHealth Belief Model HandoutRIK HAROLD GATPANDANNo ratings yet
- DSE-03-U2 - Behavior & HealthDocument23 pagesDSE-03-U2 - Behavior & HealthIndrashis MandalNo ratings yet
- Wound Care 101Document8 pagesWound Care 101French Pastolero-ManaloNo ratings yet
- ECG Taking: Electrocardiogram Taking (For Return Demonstration)Document3 pagesECG Taking: Electrocardiogram Taking (For Return Demonstration)French Pastolero-ManaloNo ratings yet
- Nclex: I Hereby Understand and Agree To The Above PolicyDocument2 pagesNclex: I Hereby Understand and Agree To The Above PolicyFrench Pastolero-ManaloNo ratings yet
- Surgical Hand Scrub: Name of Student - Steps Return Demo 1 2 PEDocument3 pagesSurgical Hand Scrub: Name of Student - Steps Return Demo 1 2 PEFrench Pastolero-ManaloNo ratings yet
- Mini Mental Status ExamDocument10 pagesMini Mental Status ExamFrench Pastolero-ManaloNo ratings yet
- Wounds and Its ComplicationsDocument4 pagesWounds and Its ComplicationsFrench Pastolero-ManaloNo ratings yet
- Cross Cult in The Wkplace Refs 3ppDocument3 pagesCross Cult in The Wkplace Refs 3ppFrench Pastolero-ManaloNo ratings yet
- NCM 114 - Ward Class - MidtermDocument35 pagesNCM 114 - Ward Class - MidtermFrench Pastolero-ManaloNo ratings yet
- Wounds and Its ComplicationsDocument4 pagesWounds and Its ComplicationsFrench Pastolero-ManaloNo ratings yet
- Wound Care 101Document8 pagesWound Care 101French Pastolero-ManaloNo ratings yet
- Mini Mental Status ExamDocument10 pagesMini Mental Status ExamFrench Pastolero-ManaloNo ratings yet
- MalpresentationDocument21 pagesMalpresentationFrench Pastolero-ManaloNo ratings yet
- Milestones Notes Cognitive Development 5-To 6-Year-Olds: Present AbsentDocument2 pagesMilestones Notes Cognitive Development 5-To 6-Year-Olds: Present AbsentFrench Pastolero-ManaloNo ratings yet
- PancreatitisDocument28 pagesPancreatitisFrench Pastolero-ManaloNo ratings yet
- Illness Behavior & PerceptionDocument30 pagesIllness Behavior & PerceptionFrench Pastolero-ManaloNo ratings yet
- More Than 100 Keyboard Shortcuts Must ReadDocument6 pagesMore Than 100 Keyboard Shortcuts Must ReadMaayans Nathas100% (1)
- Singapore AgenciesDocument2 pagesSingapore AgenciesFrench Pastolero-ManaloNo ratings yet
- Instruct Plan DescDocument3 pagesInstruct Plan DescFrench Pastolero-ManaloNo ratings yet
- Ielts Review CenterDocument4 pagesIelts Review CenterKim Andre Lopez TanNo ratings yet
- Venous-Preserving Sylvian DissectionDocument10 pagesVenous-Preserving Sylvian DissectionMorteza Mazloom Farsi BafNo ratings yet
- Shifting From Engineer To Product ManagerDocument2 pagesShifting From Engineer To Product ManagerRegin IqbalNo ratings yet
- Posse ProcessDocument4 pagesPosse Processapi-597185067No ratings yet
- Chula Vista High School's 11 Grade Portfolio Assignment ReflectionDocument2 pagesChula Vista High School's 11 Grade Portfolio Assignment Reflectionapi-450373829No ratings yet
- PANSITDocument42 pagesPANSITMaenard TambauanNo ratings yet
- Lesson 3 EdtpaDocument4 pagesLesson 3 Edtpaapi-314828591No ratings yet
- Contoh Soal Beggs and BrillDocument8 pagesContoh Soal Beggs and BrillClaviano LeiwakabessyNo ratings yet
- Grammar and StructureDocument5 pagesGrammar and StructureAini ZahraNo ratings yet
- SRM Curricula 2018 Branchwise PDFDocument110 pagesSRM Curricula 2018 Branchwise PDFrushibmr197856040% (1)
- Arusha Technical CollegeDocument4 pagesArusha Technical CollegeNamwangala Rashid NatinduNo ratings yet
- Asdmanual 1Document88 pagesAsdmanual 1api-249215481100% (1)
- Cause and Effect EssayDocument3 pagesCause and Effect EssayLilianNo ratings yet
- Group Project BY: Fatima Ahmed Fagih, Sharifah Yahya Muharish and Taghred Mohmed MnoerDocument12 pagesGroup Project BY: Fatima Ahmed Fagih, Sharifah Yahya Muharish and Taghred Mohmed Mnoerتغريد محمدNo ratings yet
- Grade 1 - Action Plan On Reading Intervention For Struggling ReadersDocument3 pagesGrade 1 - Action Plan On Reading Intervention For Struggling Readersblessy100% (2)
- Top Performing Schools Customs Broker Board Exam October 2009Document2 pagesTop Performing Schools Customs Broker Board Exam October 2009LEzNo ratings yet
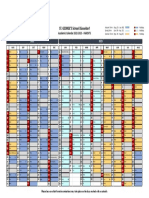
- Academic Calendar 22-23 - SGSD - PARENTS - FINALDocument1 pageAcademic Calendar 22-23 - SGSD - PARENTS - FINALfloraNo ratings yet
- Module 6Document7 pagesModule 6Johnallenson DacosinNo ratings yet
- Learn OSMDocument3 pagesLearn OSMJulian Lozano BrauNo ratings yet
- 2009-10-07 015349 Five StepDocument1 page2009-10-07 015349 Five StepAndrew PiwonskiNo ratings yet
- S R & M C P: J A S L, M O U: Management, 13 Edition Instructor ManualDocument8 pagesS R & M C P: J A S L, M O U: Management, 13 Edition Instructor ManualShahid Kalim KhanNo ratings yet
- Recruitment - P&RD, Assam PDFDocument2 pagesRecruitment - P&RD, Assam PDFPranab KumarNo ratings yet
- The Soldier's Tale Programme NotesDocument6 pagesThe Soldier's Tale Programme NotesStefano BoccacciNo ratings yet
- Coach CarterDocument3 pagesCoach Cartermichael manglicmotNo ratings yet
- T7 Curriculum Vitae For Proposed Professional Staff: Part1:Bidding ProceduresDocument136 pagesT7 Curriculum Vitae For Proposed Professional Staff: Part1:Bidding ProceduresFNo ratings yet
- TABLE OF CONTENTS FINAL - 2ndDocument10 pagesTABLE OF CONTENTS FINAL - 2ndKaren CobachaNo ratings yet