You might also like
- Fast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseFrom EverandFast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseNo ratings yet
- SGD 11 Integumentary Case 1Document14 pagesSGD 11 Integumentary Case 1Destiny Church ZamboangaNo ratings yet
- Malignant Melanoma and Skin Cancer: Igor Y. Galaychuk, MD, DSCDocument53 pagesMalignant Melanoma and Skin Cancer: Igor Y. Galaychuk, MD, DSCMohammadSAL-RawashdehNo ratings yet
- Anal Melanoma: Marc Singer, M.D. and Matthew G. Mutch, M.DDocument10 pagesAnal Melanoma: Marc Singer, M.D. and Matthew G. Mutch, M.DbkiriazovNo ratings yet
- Melanoma: Meku Damtie (M.D.) July 18, 2006Document38 pagesMelanoma: Meku Damtie (M.D.) July 18, 2006Worku KifleNo ratings yet
- Ecancermedicalscience 2017 Article 731Document8 pagesEcancermedicalscience 2017 Article 731Luis JuarezNo ratings yet
- Adenoid Cystic Carcinoma of Hard Palate: A Case ReportDocument5 pagesAdenoid Cystic Carcinoma of Hard Palate: A Case ReportHemant GuptaNo ratings yet
- Skin Lesion DiagnosisDocument9 pagesSkin Lesion DiagnosisaequNo ratings yet
- Topic: Melanoma: Case ProtocolDocument4 pagesTopic: Melanoma: Case ProtocolIC BNo ratings yet
- Case 17378: Unicentric Intra-Abdominal Castleman's Disease Mimicking MalignancyDocument8 pagesCase 17378: Unicentric Intra-Abdominal Castleman's Disease Mimicking MalignancyPedro Luis Almeyda RamírezNo ratings yet
- Subcutaneous MetsDocument27 pagesSubcutaneous MetsDavidJohnsonNo ratings yet
- Unusual Skin TumorsDocument12 pagesUnusual Skin TumorsGleny SumNo ratings yet
- Lipoblastoma Case ReportDocument10 pagesLipoblastoma Case ReportFaisal AshfaqueNo ratings yet
- Case Discussion Parotid Gland1Document25 pagesCase Discussion Parotid Gland1Rushabh YadavNo ratings yet
- History History: Past Medical History: Past Medical HistoryDocument7 pagesHistory History: Past Medical History: Past Medical HistoryAtandi JosephatNo ratings yet
- PathologyDocument58 pagesPathologysankethg93No ratings yet
- Skin Cancers. Malignant MelanomaDocument53 pagesSkin Cancers. Malignant MelanomaАбдул Насер МохаммадізмаелNo ratings yet
- Maligna MelanomaDocument80 pagesMaligna MelanomaNoveldy PitnaNo ratings yet
- Breast Cancer: Presented By: Ola NemriDocument46 pagesBreast Cancer: Presented By: Ola NemriHaitham Ahmed100% (1)
- Metastatic Malignant Melanoma: A Case StudyDocument3 pagesMetastatic Malignant Melanoma: A Case StudyDyerik LilingNo ratings yet
- Malignant Epithelial NeoplasmsDocument19 pagesMalignant Epithelial NeoplasmsAtef Mahmoud AhmedNo ratings yet
- МартDocument55 pagesМартLuisAngelPonceTorresNo ratings yet
- Skin Malignancies: By: Dr. Nang'OleDocument56 pagesSkin Malignancies: By: Dr. Nang'OleAlexNo ratings yet
- Nodular Malignant Melanoma: Case ReportDocument13 pagesNodular Malignant Melanoma: Case ReportasclepiuspdfsNo ratings yet
- Primary Angiosarcoma Breast With Intractable ThrombocytopeniaDocument4 pagesPrimary Angiosarcoma Breast With Intractable ThrombocytopeniaMuneer KhalamNo ratings yet
- Cutaneous Collision Cancers Review HUMANSDocument5 pagesCutaneous Collision Cancers Review HUMANSgranulomatous pneumoniaNo ratings yet
- Case Report DR Priti LalDocument2 pagesCase Report DR Priti LalChristopher JulienNo ratings yet
- Chronic UlcerDocument4 pagesChronic Ulcerahmed bouzouidaNo ratings yet
- Group 4 Case Study On Malignant MelanomaDocument7 pagesGroup 4 Case Study On Malignant MelanomaLance JardiolinNo ratings yet
- Squamous Cell CarcinomaDocument53 pagesSquamous Cell CarcinomaWacky BlankNo ratings yet
- Review Article: Cancers of The Appendix: Review of The LiteraturesDocument7 pagesReview Article: Cancers of The Appendix: Review of The LiteraturesMaman AhmadNo ratings yet
- Bilateral BreastDocument24 pagesBilateral Breastamrul0776No ratings yet
- Salivary Gland Tumors: 1. AdenomasDocument18 pagesSalivary Gland Tumors: 1. AdenomasMahammed Ahmed BadrNo ratings yet
- Parotid TumorDocument37 pagesParotid TumorRiyan SaputraNo ratings yet
- Publications 011Document4 pagesPublications 011utamiNo ratings yet
- Case of The Week - Spindle CellDocument33 pagesCase of The Week - Spindle Cellgovind rajNo ratings yet
- A Case Report and Literature ReviewDocument10 pagesA Case Report and Literature ReviewDerri HafaNo ratings yet
- Melanocytes, Mole, MelanomaDocument35 pagesMelanocytes, Mole, MelanomaDeba P SarmaNo ratings yet
- Diagnosis and Treatment of MelanomaDocument14 pagesDiagnosis and Treatment of MelanomaAnonymous Af24L7No ratings yet
- MelanomaDocument11 pagesMelanomaAriSeliengNo ratings yet
- Skin CancerDocument7 pagesSkin Cancerعبدالعزيز احمد علي عتشNo ratings yet
- Congenital Cystic Masses of NeckDocument47 pagesCongenital Cystic Masses of NeckFibrianti SeputriNo ratings yet
- CASE Melanoma MalignaDocument29 pagesCASE Melanoma Malignaushagi-chanNo ratings yet
- Melanoma: Edward Buckingham, M.D. Combined Plastics Conference September 6, 2000Document53 pagesMelanoma: Edward Buckingham, M.D. Combined Plastics Conference September 6, 2000Kadek Ariarta MahartamaNo ratings yet
- Case Study Breast CaDocument32 pagesCase Study Breast Caapi-391376321No ratings yet
- An Extreme Makeover Down Under - Case Report On Vulvar CarcinomaDocument44 pagesAn Extreme Makeover Down Under - Case Report On Vulvar CarcinomaLorMD34100% (1)
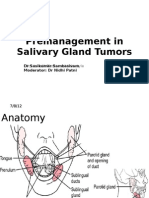
- Premanagement in Salivary Gland TumorsDocument40 pagesPremanagement in Salivary Gland TumorsDr Sasikumar SambasivamNo ratings yet
- Salivary Gland MalignanciesDocument69 pagesSalivary Gland MalignanciesKessi VikaneswariNo ratings yet
- Case Report LimfangiosarkomaDocument8 pagesCase Report Limfangiosarkomaqueen_ryNo ratings yet
- Colorectal Cancer : Presented By: Anas Jolani - Amiral Aiman - Ahmed FathiDocument55 pagesColorectal Cancer : Presented By: Anas Jolani - Amiral Aiman - Ahmed FathiRashed ShatnawiNo ratings yet
- Case Report Lung Cancer With Skin and Breast MetasDocument6 pagesCase Report Lung Cancer With Skin and Breast Metasreni melindaNo ratings yet
- Case Study 2016Document11 pagesCase Study 2016api-307778342No ratings yet
- Hidradenoma Case StudyDocument4 pagesHidradenoma Case StudyZaynaNaseemNo ratings yet
- Atypical Melanoma Mimicking A Vascular Tumor: Clinical and Dermoscopic FindingsDocument6 pagesAtypical Melanoma Mimicking A Vascular Tumor: Clinical and Dermoscopic FindingsIJAR JOURNALNo ratings yet
- Primary Excision Margins, Sentinel Lymph Node Biopsy, and Completion Lymph Node Dissection in Cutaneous MelanomaDocument10 pagesPrimary Excision Margins, Sentinel Lymph Node Biopsy, and Completion Lymph Node Dissection in Cutaneous MelanomaAndrés Faúndez TeránNo ratings yet
- Carcinosarcoma of The Parotid Gland: Case ReportDocument42 pagesCarcinosarcoma of The Parotid Gland: Case ReportrohinmNo ratings yet
- DR 180114164748Document43 pagesDR 180114164748Hasnain ToheedNo ratings yet
- Bab TerakirDocument86 pagesBab TerakirDian Asri Gumilang PratiwiNo ratings yet
- 1991 - Nonhealing Leg Ulcers - A Manifestation of Basal Cell - carCInomaDocument3 pages1991 - Nonhealing Leg Ulcers - A Manifestation of Basal Cell - carCInomaAnca Catalina MunteanuNo ratings yet
- Branches of ZoologyDocument3 pagesBranches of ZoologyVivek Morya100% (1)
- Integrated Application Form 97 2003 Compatible PDFDocument15 pagesIntegrated Application Form 97 2003 Compatible PDFdrchughNo ratings yet
- CV Stoskopf 12 06Document52 pagesCV Stoskopf 12 06shinevoiceNo ratings yet
- Carrubba Botanical Guide RDocument247 pagesCarrubba Botanical Guide Rafridikhanjan100% (3)
- Microbiology 3M All 333Document55 pagesMicrobiology 3M All 333deeksha.ivannaNo ratings yet
- Respiratory Failure in Children PDFDocument47 pagesRespiratory Failure in Children PDFOxana TurcuNo ratings yet
- LT 2 Members: Raazia Jalil, Ali Amjad & Ali Raza: Project 2 Doctors InterviewDocument3 pagesLT 2 Members: Raazia Jalil, Ali Amjad & Ali Raza: Project 2 Doctors InterviewfatimaNo ratings yet
- L10 ToleranceDocument19 pagesL10 Tolerancesara garciaNo ratings yet
- Curriculum Vitae of Dr. Ankur BaruaDocument38 pagesCurriculum Vitae of Dr. Ankur BaruaANKUR BARUA100% (1)
- Msds Nano PolishDocument5 pagesMsds Nano PolishGan LordNo ratings yet
- WEB VTH 01292009Document28 pagesWEB VTH 01292009Dave L100% (1)
- Acog Embarazo Gemelar 2004 PDFDocument15 pagesAcog Embarazo Gemelar 2004 PDFEliel MarcanoNo ratings yet
- MDMA PowerpointDocument16 pagesMDMA Powerpointapi-26938624No ratings yet
- Phenylephrine HydrochlorideDocument5 pagesPhenylephrine HydrochlorideRoger Jr PumarenNo ratings yet
- Medication BookDocument448 pagesMedication BookAlbert ChuwaNo ratings yet
- Prosedur Manual PlasentahjhjjhkjkjDocument15 pagesProsedur Manual PlasentahjhjjhkjkjMif Al-HudaNo ratings yet
- MSDS Refrigerant R407CDocument8 pagesMSDS Refrigerant R407Chambali bimatamaNo ratings yet
- Blood Typing GameDocument4 pagesBlood Typing GameWidjaya HS TeacherNo ratings yet
- NCP Ineffective Airway Clearance Related To Lung Impairment PNEUMOTHORAXDocument5 pagesNCP Ineffective Airway Clearance Related To Lung Impairment PNEUMOTHORAXMa. Elaine Carla Tating0% (2)
- Fucidin® OintDocument1 pageFucidin® OintIanthe SinghNo ratings yet
- Pharma Biotech M A Transactions 2005-2012Document13 pagesPharma Biotech M A Transactions 2005-2012Aniket ApteNo ratings yet
- Family Therapy For Autism Spectrum Disorders (Cto)Document21 pagesFamily Therapy For Autism Spectrum Disorders (Cto)Julie Rose AlboresNo ratings yet
- Anexo 3 Consenso de La Eskka en OsteoartritisDocument58 pagesAnexo 3 Consenso de La Eskka en OsteoartritisgrimmNo ratings yet
- Foundations Study Guide FINAL EXAMDocument15 pagesFoundations Study Guide FINAL EXAMigorot89100% (1)
- Tai Chi LiteratureDocument2 pagesTai Chi LiteratureMichael Fong100% (1)
- J&J CompanyDocument127 pagesJ&J CompanyRam TyagiNo ratings yet
- MBB 1 Handout 1 and What About BiotechnologyDocument4 pagesMBB 1 Handout 1 and What About BiotechnologyMariah Shanice BasaNo ratings yet
- Tinnitus EpidemiologyDocument149 pagesTinnitus EpidemiologyTheodoros Kontogiannis100% (1)
- BestDocument25 pagesBestAlejandro Lopez OsorioNo ratings yet
- Reverse TsaDocument4 pagesReverse Tsaprwill00No ratings yet