You might also like
- DrugsDocument6 pagesDrugsDante Bacud Formoso IIINo ratings yet
- Ra 9165 Handout-E Drug & Drug TestingDocument5 pagesRa 9165 Handout-E Drug & Drug TestingFait HeeNo ratings yet
- Transported Within 2 Hours of Collected Leak-Proof Plastic Bags With A Permanent SealDocument5 pagesTransported Within 2 Hours of Collected Leak-Proof Plastic Bags With A Permanent SealMarlonZunigaNo ratings yet
- Historical Perspective, Different Phases of Clinical TrialsDocument16 pagesHistorical Perspective, Different Phases of Clinical Trialsexcel proNo ratings yet
- DCS CR Final Exam Question FileDocument23 pagesDCS CR Final Exam Question FileAnish RedkarNo ratings yet
- CLINICAL PRACTICUM Activity Book Revised 2014Document17 pagesCLINICAL PRACTICUM Activity Book Revised 2014helpNo ratings yet
- Differential Diagnosis of Body Fluids in Small Animal CytologyFrom EverandDifferential Diagnosis of Body Fluids in Small Animal CytologyNo ratings yet
- M. Pharm II Sem Clinical Trials and PV Assignment 8 Name: Roll NoDocument4 pagesM. Pharm II Sem Clinical Trials and PV Assignment 8 Name: Roll NoAkhil BhatnagarNo ratings yet
- UCM397228 Pharmaceutical Microbiology ManualDocument91 pagesUCM397228 Pharmaceutical Microbiology Manualnsk79in@gmail.com100% (1)
- Ir CDC Bioassay enDocument28 pagesIr CDC Bioassay enAde margusNo ratings yet
- Lab Policy and ProceduresDocument8 pagesLab Policy and ProceduresvasanthrsciwiaNo ratings yet
- June 3, 2022 Summary Basis For Regulatory Action - PRIORIXDocument31 pagesJune 3, 2022 Summary Basis For Regulatory Action - PRIORIXjaikp56No ratings yet
- Specimen Collections in The Medical Microbiology and ParasitologyNOTESDocument64 pagesSpecimen Collections in The Medical Microbiology and ParasitologyNOTESPrincewill SeiyefaNo ratings yet
- CCWS™ Candida Cell Wall Suppressor Study ReviewDocument16 pagesCCWS™ Candida Cell Wall Suppressor Study ReviewCCWS Candida Cleanser Treatment Protocol100% (1)
- Pharmacological Screening Methods & Toxicology: Revised & UpdatedFrom EverandPharmacological Screening Methods & Toxicology: Revised & UpdatedRating: 4.5 out of 5 stars4.5/5 (11)
- 3.3 Specimen Collection and ProcessingDocument29 pages3.3 Specimen Collection and ProcessingTobio KunnyNo ratings yet
- Pharmacuetical Microbiology Manual 2014 PDFDocument86 pagesPharmacuetical Microbiology Manual 2014 PDFteaNo ratings yet
- Skeletal Examination by Alizarin StainingDocument617 pagesSkeletal Examination by Alizarin StainingromelNo ratings yet
- PMLS Lesson 89Document2 pagesPMLS Lesson 89Riza Andrea Joy QuietaNo ratings yet
- Good Clinical Practices Concepts and Case Studies Kim IsaacsDocument21 pagesGood Clinical Practices Concepts and Case Studies Kim IsaacsChandra Shekar GNo ratings yet
- Lab Values: An Easy Guide to Learn Everything You Need to Know About Laboratory Medicine and Its Relevance in Diagnosing DiseaseFrom EverandLab Values: An Easy Guide to Learn Everything You Need to Know About Laboratory Medicine and Its Relevance in Diagnosing DiseaseRating: 5 out of 5 stars5/5 (2)
- Assesment Tool Policies and ProceduresDocument3 pagesAssesment Tool Policies and Procedureslemar aribalNo ratings yet
- Checklist of Pathology Laboratory and Its Quality Indicators For NABH Accreditation PreparationDocument3 pagesChecklist of Pathology Laboratory and Its Quality Indicators For NABH Accreditation PreparationQUALITY SIDARTH HOSPITALS100% (1)
- RKS Savello 101007Document49 pagesRKS Savello 101007Ani SharmaNo ratings yet
- 4 1Document14 pages4 1md.wahiduzzamanjewel412No ratings yet
- Sathern SubpoenaDocument36 pagesSathern SubpoenamikekvolpeNo ratings yet
- Kirby Bauer Disc DiffusionDocument9 pagesKirby Bauer Disc DiffusionSubhradeep GhoshNo ratings yet
- Program April 2024 PHLEDocument4 pagesProgram April 2024 PHLETheSummitExpressNo ratings yet
- Forensic 3 3Document19 pagesForensic 3 3argiebutchconcha0715No ratings yet
- Niamh MarieDocument299 pagesNiamh MarieS291991No ratings yet
- Thomas Anthony Munro - The Chemistry of Salvia DivinorumDocument283 pagesThomas Anthony Munro - The Chemistry of Salvia DivinorumnnnnjwNo ratings yet
- Health AssessmentDocument73 pagesHealth AssessmentKristil ChavezNo ratings yet
- 1.confirm Information in Report 2.investigate and Collect DataDocument15 pages1.confirm Information in Report 2.investigate and Collect DataAsmi MohamedNo ratings yet
- Abg Analysis Performance ChecklistDocument8 pagesAbg Analysis Performance ChecklistMhel MGNo ratings yet
- Checklist of Pathology Laboratory and Its Quality Indicators For NABH Accreditation PreparationDocument3 pagesChecklist of Pathology Laboratory and Its Quality Indicators For NABH Accreditation PreparationPayal Thakker100% (1)
- Molecular Biological and Immunological Techniques and Applications for Food ChemistsFrom EverandMolecular Biological and Immunological Techniques and Applications for Food ChemistsBert PoppingNo ratings yet
- Analytical MicrobiologyFrom EverandAnalytical MicrobiologyFrederick KavanaghNo ratings yet
- Document 1Document17 pagesDocument 1Chelzea EhurangoNo ratings yet
- Aubf Outline EditedDocument16 pagesAubf Outline EditedNoraine Princess TabangcoraNo ratings yet
- BioassayszzDocument86 pagesBioassayszzNotfor TaoNo ratings yet
- Test Bank For Tietz Fundamentals of Clinical Chemistry and Molecular Diagnostics 7th Edition by BurtisDocument35 pagesTest Bank For Tietz Fundamentals of Clinical Chemistry and Molecular Diagnostics 7th Edition by Burtiscereus.kailc39cf97% (38)
- 3 - Clinical LaboratoryDocument12 pages3 - Clinical Laboratorysabir osman100% (1)
- Defining The Practice of Medical TechnologyDocument47 pagesDefining The Practice of Medical TechnologyCharles Ian OliquinoNo ratings yet
- Recommended Methods For The Identification and Analysis of Piperazines in Seized Materials (2013)Document56 pagesRecommended Methods For The Identification and Analysis of Piperazines in Seized Materials (2013)Luděk SpurnýNo ratings yet
- Diagnostic ProceduresDocument10 pagesDiagnostic Proceduresmc gallegoNo ratings yet
- Review Questions Unit 1 AnswerDocument4 pagesReview Questions Unit 1 Answerkoket negashNo ratings yet
- Drs Masrial Mahyudin Apt - Materi Teknik Pencampuran Obat Khemo & Iv - 7 Okt 2022Document56 pagesDrs Masrial Mahyudin Apt - Materi Teknik Pencampuran Obat Khemo & Iv - 7 Okt 2022Opi RofidinNo ratings yet
- Checklist 7 Step of Occupational Diagnosis - 2021-2022Document4 pagesChecklist 7 Step of Occupational Diagnosis - 2021-2022wahyu kijang ramadhanNo ratings yet
- Cell Counting ProformaDocument5 pagesCell Counting ProformadonaNo ratings yet
- MEDL499 - Medical Lab Internship Program - Guidelines - Fall 2022Document31 pagesMEDL499 - Medical Lab Internship Program - Guidelines - Fall 2022Fatima Al IssaNo ratings yet
- SafariDocument10 pagesSafariشمايل الجهنيNo ratings yet
- 5 Thomas Hammack PDFDocument38 pages5 Thomas Hammack PDFAbhishek BanerjeeNo ratings yet
- ABMM Sample QuestionsDocument7 pagesABMM Sample QuestionsRanjit Kumar ShahNo ratings yet
- Chemistry 422 BIOCHEMISTRY LABORATORY MADocument142 pagesChemistry 422 BIOCHEMISTRY LABORATORY MAangelita aquinoNo ratings yet
- Drummelsmith - Laboratory Diagnosis and Bacterial Identification - Study GuideDocument19 pagesDrummelsmith - Laboratory Diagnosis and Bacterial Identification - Study GuideTom TsouNo ratings yet
- Training Report On Biochemical Assay and Bio Instrumention.: Anugarah Narayan College, Patna (Bihar)Document38 pagesTraining Report On Biochemical Assay and Bio Instrumention.: Anugarah Narayan College, Patna (Bihar)Friends ZoneNo ratings yet
- Post Trial Review Procedures in Military Court MartialsDocument2 pagesPost Trial Review Procedures in Military Court MartialsMichael Waddington100% (1)
- Types of Courts MartialDocument2 pagesTypes of Courts MartialMichael Waddington100% (1)
- Command Disciplinary OptionsDocument1 pageCommand Disciplinary OptionsMichael WaddingtonNo ratings yet
- Appellate Court ReviewDocument2 pagesAppellate Court ReviewMichael WaddingtonNo ratings yet
- Release of Information Privacy ActDocument5 pagesRelease of Information Privacy ActMichael WaddingtonNo ratings yet
- Summary Court MartialDocument1 pageSummary Court MartialMichael WaddingtonNo ratings yet
- General Court MartialDocument1 pageGeneral Court MartialMichael WaddingtonNo ratings yet
- The Uniform Code of Military Justice and Manual For Courts-MartialDocument3 pagesThe Uniform Code of Military Justice and Manual For Courts-MartialMichael Waddington100% (1)
- Article 32 InvestigationsDocument3 pagesArticle 32 InvestigationsMichael WaddingtonNo ratings yet
- Command Options For Handling MisconductDocument2 pagesCommand Options For Handling MisconductMichael WaddingtonNo ratings yet
- Nonjudicial PunishmentDocument2 pagesNonjudicial PunishmentMichael Waddington100% (1)
- Pretrial Confinement in The MilitaryDocument2 pagesPretrial Confinement in The MilitaryMichael Waddington100% (1)
- Suspect RightsDocument1 pageSuspect RightsMichael Waddington100% (1)
- Military Court Martial JurisdictionDocument4 pagesMilitary Court Martial JurisdictionMichael Waddington100% (1)
- Unlawful Command InfluenceDocument2 pagesUnlawful Command InfluenceMichael Waddington100% (2)
- Officer Resignation Fact SheetDocument2 pagesOfficer Resignation Fact SheetMichael Waddington100% (1)
- Clemency Parole PardonsDocument1 pageClemency Parole PardonsMichael WaddingtonNo ratings yet
- Discharges Resignations and Retirements in Lieu of Court MartialDocument2 pagesDischarges Resignations and Retirements in Lieu of Court MartialMichael WaddingtonNo ratings yet
- Command Disciplinary OptionsDocument1 pageCommand Disciplinary OptionsMichael WaddingtonNo ratings yet
- Comparison To The Civilian Preliminary Hearing and Grand Jury ProcessDocument2 pagesComparison To The Civilian Preliminary Hearing and Grand Jury ProcessMichael Waddington100% (1)
- Clemency Parole PardonsDocument1 pageClemency Parole PardonsMichael WaddingtonNo ratings yet
- A Recent Review On Technological Advancement and The Use of Natural Superdisintegrant in The Formulation of Fast Disintegrating TabletDocument7 pagesA Recent Review On Technological Advancement and The Use of Natural Superdisintegrant in The Formulation of Fast Disintegrating TabletYudi GugupNo ratings yet
- Chemistry in Everyday Life MCQSDocument3 pagesChemistry in Everyday Life MCQSAyush RajNo ratings yet
- Paracetamol (Alvedon) Acetylcysteine Fluimucil KCL (Kalium Durule)Document1 pageParacetamol (Alvedon) Acetylcysteine Fluimucil KCL (Kalium Durule)Jesse James Advincula EdjecNo ratings yet
- CostPlusDrugs - Price List - 20230412Document66 pagesCostPlusDrugs - Price List - 20230412CBS 11 NewsNo ratings yet
- Bioavailability of DrugsDocument17 pagesBioavailability of DrugsDua waheedNo ratings yet
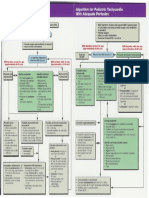
- Pediatric Tachycardia AlgorithmsDocument1 pagePediatric Tachycardia AlgorithmsGalih FatoniNo ratings yet
- Drug Study-Ceftriaxone ClindamycinDocument2 pagesDrug Study-Ceftriaxone ClindamycinDavid VillanuevaNo ratings yet
- Industrial Training3Document13 pagesIndustrial Training3ArshNo ratings yet
- Case - Study - 2-A Fall RiskDocument4 pagesCase - Study - 2-A Fall Risksavvy_as_98-1No ratings yet
- Drugs and Cosmetics Act 1940, Rule 1945 by Dr. Izhar AhmadDocument49 pagesDrugs and Cosmetics Act 1940, Rule 1945 by Dr. Izhar AhmadijharNo ratings yet
- NarcoticsDocument6 pagesNarcoticsanaeshkl100% (1)
- Epilepsy Guideline in AdultsDocument131 pagesEpilepsy Guideline in AdultsNEuRoLoGisT CoFFeeCuP100% (3)
- Formulary 2009Document51 pagesFormulary 2009Wen ZhuNo ratings yet
- Drug StudyDocument5 pagesDrug StudyRai D. MacapantonNo ratings yet
- Daily Skilled Documentation GuidelineDocument2 pagesDaily Skilled Documentation GuidelineJoanne CareahNo ratings yet
- Inlay Tablets A Novel Approach PDFDocument10 pagesInlay Tablets A Novel Approach PDFTakeshi MondaNo ratings yet
- Drug Interaction Chart PrescriptionDocument7 pagesDrug Interaction Chart PrescriptionSimona LipanNo ratings yet
- Sulfa Nil Amide Deaths of 1937Document4 pagesSulfa Nil Amide Deaths of 1937api-3810976No ratings yet
- Inserting Iv Cannula Utilizing Dummy ArmDocument6 pagesInserting Iv Cannula Utilizing Dummy ArmAnonymous B0c72x2No ratings yet
- 2018 DPRI Booklet Nov-19-18Document34 pages2018 DPRI Booklet Nov-19-18Michelle Anne Ramirez GalangaNo ratings yet
- Standarisari ObatDocument28 pagesStandarisari Obatmelisa memelNo ratings yet
- 2 DdaDocument38 pages2 DdaEdd Monzon Delamide100% (1)
- Drug Deaths in Jefferson County 2015Document16 pagesDrug Deaths in Jefferson County 2015Jeremy W. Gray100% (1)
- 2011 07 PHARMA Prescription WritingDocument8 pages2011 07 PHARMA Prescription WritingdtimtimanNo ratings yet
- Study Guide For Fluid and Electrolyte ImbalancesDocument5 pagesStudy Guide For Fluid and Electrolyte ImbalancesMandi Goetz HarmonNo ratings yet
- At The Doctors Multiple Choice Tests - 67890Document1 pageAt The Doctors Multiple Choice Tests - 67890guest470% (2)
- Neonatal Drugs Section Fifth Edition2012 PDFDocument163 pagesNeonatal Drugs Section Fifth Edition2012 PDFAhmed MohammedNo ratings yet
- FDA Pregnancy CategoriesDocument3 pagesFDA Pregnancy CategoriesHibiryen100% (1)
- 861 Drug Prescribing For Dentistry 2 Web 2 Email PDFDocument94 pages861 Drug Prescribing For Dentistry 2 Web 2 Email PDFRaphaela TravassosNo ratings yet
- Multiple IV Bolus AdministrationDocument21 pagesMultiple IV Bolus AdministrationIka NurzijahNo ratings yet