You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Protein MicroarrayDocument8 pagesProtein MicroarrayItrux JonathanNo ratings yet
- Short Communication: ChromatographyDocument6 pagesShort Communication: ChromatographyItrux JonathanNo ratings yet
- Lysis of Red Blood CellsDocument1 pageLysis of Red Blood CellsItrux JonathanNo ratings yet
- Gelatin Zymography For Detection of Matrixmetalloproteinase-2 and - 9 (MMP-2, MMP-9) From Myocardiam SamplesDocument21 pagesGelatin Zymography For Detection of Matrixmetalloproteinase-2 and - 9 (MMP-2, MMP-9) From Myocardiam SamplesItrux JonathanNo ratings yet
- Membrane Filtration Handbook Osmonics - Practical Tips and HintsDocument129 pagesMembrane Filtration Handbook Osmonics - Practical Tips and HintsItrux JonathanNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 01 - A Note On Introduction To E-Commerce - 9march2011Document12 pages01 - A Note On Introduction To E-Commerce - 9march2011engr_amirNo ratings yet
- Object-Oriented Design Patterns in The Kernel, Part 2 (LWN - Net)Document15 pagesObject-Oriented Design Patterns in The Kernel, Part 2 (LWN - Net)Rishabh MalikNo ratings yet
- Frequency Response For Control System Analysis - GATE Study Material in PDFDocument7 pagesFrequency Response For Control System Analysis - GATE Study Material in PDFNarendra AgrawalNo ratings yet
- Eng21 (Story of Hamguchi Gohei)Document9 pagesEng21 (Story of Hamguchi Gohei)Alapan NandaNo ratings yet
- REAL BABY FOOD: Easy All-Natural Recipes For Your Baby and Toddler by Jenna HelwigDocument8 pagesREAL BABY FOOD: Easy All-Natural Recipes For Your Baby and Toddler by Jenna HelwigHoughton Mifflin Harcourt Cookbooks50% (2)
- Better Photography - April 2018 PDFDocument100 pagesBetter Photography - April 2018 PDFPeter100% (1)
- Advent Wreath Lesson PlanDocument2 pagesAdvent Wreath Lesson Planapi-359764398100% (1)
- Resume NetezaDocument5 pagesResume Netezahi4149No ratings yet
- Conveyor Control Using Programmable Logic ControllerDocument7 pagesConveyor Control Using Programmable Logic ControllerWann RexroNo ratings yet
- A - PAGE 1 - MergedDocument73 pagesA - PAGE 1 - MergedGenalyn DomantayNo ratings yet
- Estate TaxDocument10 pagesEstate TaxCharrie Grace PabloNo ratings yet
- M.Plan SYLLABUS 2022-24Document54 pagesM.Plan SYLLABUS 2022-24Mili DawsonNo ratings yet
- Unit 4Document15 pagesUnit 4David Lopez LaraNo ratings yet
- Building For The Environment 1Document3 pagesBuilding For The Environment 1api-133774200No ratings yet
- Ideal Gas Law Lesson Plan FinalDocument5 pagesIdeal Gas Law Lesson Plan FinalLonel SisonNo ratings yet
- Bag Technique and Benedict ToolDocument2 pagesBag Technique and Benedict ToolAriel Delos Reyes100% (1)
- IBPS Clerk Pre QUANT Memory Based 2019 QuestionsDocument8 pagesIBPS Clerk Pre QUANT Memory Based 2019 Questionsk vinayNo ratings yet
- Product Specifications Product Specifications: LLPX411F LLPX411F - 00 - V1 V1Document4 pagesProduct Specifications Product Specifications: LLPX411F LLPX411F - 00 - V1 V1David MooneyNo ratings yet
- Stewart, Mary - The Little BroomstickDocument159 pagesStewart, Mary - The Little BroomstickYunon100% (1)
- Ubi Caritas Guitar Solo Arrangement by Patrick Glenn BalanzaDocument8 pagesUbi Caritas Guitar Solo Arrangement by Patrick Glenn BalanzaPatrick Glenn BalanzaNo ratings yet
- AcousticsDocument122 pagesAcousticsEclipse YuNo ratings yet
- IFR CalculationDocument15 pagesIFR CalculationSachin5586No ratings yet
- Discrete Mathematics and Its Applications: Basic Structures: Sets, Functions, Sequences, and SumsDocument61 pagesDiscrete Mathematics and Its Applications: Basic Structures: Sets, Functions, Sequences, and SumsBijori khanNo ratings yet
- BECIL Registration Portal: How To ApplyDocument2 pagesBECIL Registration Portal: How To ApplySoul BeatsNo ratings yet
- Research Paper On Air QualityDocument4 pagesResearch Paper On Air Qualityluwahudujos3100% (1)
- Specification Sheet: Case I Case Ii Operating ConditionsDocument1 pageSpecification Sheet: Case I Case Ii Operating ConditionsKailas NimbalkarNo ratings yet
- Rockwell Collins RDRDocument24 pagesRockwell Collins RDRMatty Torchia100% (5)
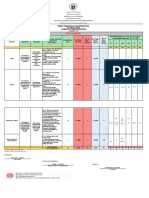
- Revised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10Document6 pagesRevised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10May Ann GuintoNo ratings yet
- 1 - Laminar and Turbulent Flow - MITWPU - HP - CDK PDFDocument13 pages1 - Laminar and Turbulent Flow - MITWPU - HP - CDK PDFAbhishek ChauhanNo ratings yet
- International Patient Referral - Part 2 - Revised - 29-04-2010 - 2Document2 pagesInternational Patient Referral - Part 2 - Revised - 29-04-2010 - 2Fatah AssadNo ratings yet