You might also like
- W1T0003XQ Combat Conditioning ConceptsDocument44 pagesW1T0003XQ Combat Conditioning ConceptsArnold ArceoNo ratings yet
- Medical Assistant Study GuideDocument116 pagesMedical Assistant Study GuideErns Jean-baptiste100% (11)
- Physical Education and Health 4 ModuleDocument38 pagesPhysical Education and Health 4 ModuleLouise ArellanoNo ratings yet
- Heat Stress PlanDocument34 pagesHeat Stress Plan01095902062ahmedNo ratings yet
- Heat StrokeDocument22 pagesHeat StrokeCrizza Maglasang100% (1)
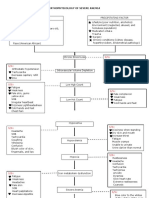
- Pathophysiology of Severe AnemiaDocument3 pagesPathophysiology of Severe AnemiaChrizley Shawn DeroniaNo ratings yet
- Exotic Animal Emergency and Critical Care MedicineDocument948 pagesExotic Animal Emergency and Critical Care MedicineCamila Garcia RodriguesNo ratings yet
- Case AnalysisDocument25 pagesCase AnalysisGerly LagutingNo ratings yet
- NP of Acute Calculous CholecystitisDocument19 pagesNP of Acute Calculous CholecystitisIris Caberte100% (1)
- Hyperthermia: Date/Hour Focus Progress NotesDocument11 pagesHyperthermia: Date/Hour Focus Progress NotesCai Sumayod Delloro100% (3)
- Apurba Das, R Alagirusamy - Science in Clothing Comfort (Woodhead Publishing India) - Woodhead Publishing (2011)Document185 pagesApurba Das, R Alagirusamy - Science in Clothing Comfort (Woodhead Publishing India) - Woodhead Publishing (2011)VenkyNo ratings yet
- Perioperative Nursing TR PDFDocument94 pagesPerioperative Nursing TR PDFKoleen Kirsten100% (1)
- Nursin Care Plan For GastroenteritisDocument7 pagesNursin Care Plan For GastroenteritisSheana Tmpl100% (2)
- Gordon's Functional Health PatternDocument5 pagesGordon's Functional Health PatternnerlynNo ratings yet
- NCP Proper CholecystectomyDocument2 pagesNCP Proper CholecystectomyGail Lian SantosNo ratings yet
- NCP UreteroDocument1 pageNCP UreteroCerie Anne OlayNo ratings yet
- Cu 3 Week 3Document3 pagesCu 3 Week 3Maica LectanaNo ratings yet
- Nursing Care PlanDocument13 pagesNursing Care Planyumiko0% (1)
- 2 Nursing-Process-in-the-care-of-the-Community - FGBDocument41 pages2 Nursing-Process-in-the-care-of-the-Community - FGBKim Bok JooNo ratings yet
- EthicsDocument1 pageEthicsNadineNo ratings yet
- NCP PainDocument1 pageNCP PaindwightciderNo ratings yet
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPRomel BaliliNo ratings yet
- B00K 3 Unit 13Document11 pagesB00K 3 Unit 13Rolli SptNo ratings yet
- Huntingtons Disease NCPDocument4 pagesHuntingtons Disease NCPJerich Mark SalasNo ratings yet
- Leptospirosis CaseDocument29 pagesLeptospirosis CaseJp RectraNo ratings yet
- Osteosarcoma-Ana and PhysiologyDocument4 pagesOsteosarcoma-Ana and PhysiologyNeirfla WassabiNo ratings yet
- 12 NCPDocument3 pages12 NCPKate ChavezNo ratings yet
- Risk For Falls As Evidence by Loss of BalanceDocument4 pagesRisk For Falls As Evidence by Loss of BalanceAlexandrea MayNo ratings yet
- College of Nursing and Allied Medical Sciences: WesleyanDocument3 pagesCollege of Nursing and Allied Medical Sciences: WesleyanPrince Juzzel Banag100% (1)
- CholelithiasisDocument6 pagesCholelithiasismarkzamNo ratings yet
- Stomach CancerDocument7 pagesStomach CancerSyazmin KhairuddinNo ratings yet
- Aiza NCPDocument6 pagesAiza NCPponponolmedoNo ratings yet
- Acute Appendicitis Group CDocument40 pagesAcute Appendicitis Group CHeart TolenadaNo ratings yet
- Epoetin AlfaDocument3 pagesEpoetin Alfaapi-3797941No ratings yet
- 4 THE PARTNERSHIP APPROACH TO COMMUNITY HEALTH PRACTICE Mam ThaiDocument14 pages4 THE PARTNERSHIP APPROACH TO COMMUNITY HEALTH PRACTICE Mam ThaiKasandra Dawn Moquia BerisoNo ratings yet
- HERNIADocument27 pagesHERNIAVanessa SumalbagNo ratings yet
- Fitrawati Arifuddin - Nursing Care Plan Deficiency of Fluid VolumeDocument12 pagesFitrawati Arifuddin - Nursing Care Plan Deficiency of Fluid VolumefitrawatiarifuddinNo ratings yet
- NCPDocument4 pagesNCPJahmie RiveraNo ratings yet
- NCPDocument6 pagesNCPBon BonNo ratings yet
- CASE STUDY PheumoniaDocument5 pagesCASE STUDY PheumoniaEdelweiss Marie CayetanoNo ratings yet
- Propranolol 1 PresentationDocument17 pagesPropranolol 1 Presentationapi-284092317100% (1)
- Geria Rle Week 6 Pain 1Document1 pageGeria Rle Week 6 Pain 1Maica LectanaNo ratings yet
- Philippine Nursing Organizations Org Name DescriptionDocument8 pagesPhilippine Nursing Organizations Org Name DescriptionShehada Marcos BondadNo ratings yet
- Learning Feedback g2Document8 pagesLearning Feedback g2Darwin DaveNo ratings yet
- I. Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationDocument4 pagesI. Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationCherubim Lei DC FloresNo ratings yet
- HernioplastyDocument6 pagesHernioplastyCherry Delos ReyesNo ratings yet
- Epidemiology and Pathophysiology of Colonic Diverticular DiseaseDocument8 pagesEpidemiology and Pathophysiology of Colonic Diverticular DiseaseAnonymous Hz5w55No ratings yet
- Drug StudyDocument3 pagesDrug StudyLorraine Tuesday BuenviajeNo ratings yet
- Reflection On Feeding Elderly ClientsDocument2 pagesReflection On Feeding Elderly ClientsLaydee GiaAmNo ratings yet
- NCP TetanusDocument2 pagesNCP TetanusSugar Capule - Manuel0% (1)
- D."Parang Giniginaw Man Ako" As Verbalized, Patient CoversDocument1 pageD."Parang Giniginaw Man Ako" As Verbalized, Patient CoversSherena NicolasNo ratings yet
- Assignment For Oxy. Online BasedDocument5 pagesAssignment For Oxy. Online BasedNurhassem Nor AkangNo ratings yet
- 6 Nursing Care Plan 1Document2 pages6 Nursing Care Plan 1Denise Louise PoNo ratings yet
- Concept Map - Colon CancerDocument2 pagesConcept Map - Colon Cancerbea pegadNo ratings yet
- Nursing Care of Uremic SyndromeDocument11 pagesNursing Care of Uremic Syndromeyoedha_banditozz50% (2)
- NCP ProperDocument9 pagesNCP Properstephanie eduarteNo ratings yet
- Pathophysiology of Transitional Cell CarcinomaDocument10 pagesPathophysiology of Transitional Cell CarcinomaJheanAlphonsineT.MeansNo ratings yet
- ScriptDocument12 pagesScriptWaleed Nadeem50% (2)
- AcknowledgementDocument9 pagesAcknowledgementjhzenNo ratings yet
- Decreased Cardiac OutputDocument1 pageDecreased Cardiac OutputPrecious Heart Sotero TababaNo ratings yet
- Impaired Gas ExchangeDocument10 pagesImpaired Gas ExchangeWardinatul ImanNo ratings yet
- Case File GERDDocument9 pagesCase File GERDMutiara Shifa100% (1)
- Pathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsDocument4 pagesPathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsLovely DaroleNo ratings yet
- Goal Not MetDocument4 pagesGoal Not MetAyaBasilioNo ratings yet
- NCP AnxietyDocument1 pageNCP AnxietyUnang MagnayeNo ratings yet
- PYOMYOSITISDocument6 pagesPYOMYOSITISChristine CoridoNo ratings yet
- NURSING CARE PLAN FOR CROHN'sDocument2 pagesNURSING CARE PLAN FOR CROHN'sMuhyeeSalaIdjadNo ratings yet
- Oks Na To Thank U Aubs!!: Okiii!!! Wuv U All!Document10 pagesOks Na To Thank U Aubs!!: Okiii!!! Wuv U All!CiaraNo ratings yet
- SAMPLE Case PresentationDocument4 pagesSAMPLE Case PresentationRachel NiuNo ratings yet
- Jessica First Aid PPDocument22 pagesJessica First Aid PPGilmarie RomitaresNo ratings yet
- Energy DrinksDocument3 pagesEnergy DrinksNuc LeusNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanCspc Crcyc50% (2)
- GULF - HS.GUIDE05-Safe Working in The Heat Checklist-Rev01Document1 pageGULF - HS.GUIDE05-Safe Working in The Heat Checklist-Rev01HamoudaNo ratings yet
- Current Ratite Therapy: General Principles of TherapyDocument18 pagesCurrent Ratite Therapy: General Principles of Therapyali hendyNo ratings yet
- Health Group3Document29 pagesHealth Group3Angela OrenseNo ratings yet
- NCP For HYPERTHERMIADocument3 pagesNCP For HYPERTHERMIAGil Ganiban0% (1)
- PDHPE NotesDocument30 pagesPDHPE Notesvtfrb5rgn9No ratings yet
- Heat Index Chart: by Temperature (F) and Relative Humidity (%)Document1 pageHeat Index Chart: by Temperature (F) and Relative Humidity (%)Olga KardashNo ratings yet
- Hot and Cold Emergencies, Bites, Shock and ChokingDocument100 pagesHot and Cold Emergencies, Bites, Shock and ChokingErdem AltunNo ratings yet
- Deep Creek Planning Package Leaders PackDocument44 pagesDeep Creek Planning Package Leaders Packapi-527274757No ratings yet
- Night FeverDocument5 pagesNight FeverdewioktaNo ratings yet
- TBT 29 Hot WeatherDocument2 pagesTBT 29 Hot WeatherfrancisNo ratings yet
- Nursing Care Plan Juvida, Clarissa A. BSN 2A: "Mainit Ang Anak Ko at Nanghihina ."Document3 pagesNursing Care Plan Juvida, Clarissa A. BSN 2A: "Mainit Ang Anak Ko at Nanghihina ."Clarissa JuvidaNo ratings yet
- Heat ExhaustionDocument4 pagesHeat Exhaustionapi-356829966No ratings yet
- Personal Safety and StandardDocument13 pagesPersonal Safety and StandardGilbert ObingNo ratings yet
- Impact of Heat Stress On Poultry ProductionDocument19 pagesImpact of Heat Stress On Poultry ProductionGabriela MartinsNo ratings yet
- Heat Stroke: Review Open AccessDocument8 pagesHeat Stroke: Review Open AccessJulian HuningkorNo ratings yet
- Pool Heater Installation, Operation and Maintenance: ModelsDocument16 pagesPool Heater Installation, Operation and Maintenance: ModelsFernando ChipantasiNo ratings yet
- OptimDocument6 pagesOptimHernan emmanuel “Bart” García RamónNo ratings yet