You might also like
- Medical Terminology AssignmentDocument4 pagesMedical Terminology AssignmentBeverly GraciousNo ratings yet
- (Comprehensive Gynecology and Obstetrics) Mikio Mikami - Surgery For Gynecologic Cancer-Springer Singapore (2019)Document428 pages(Comprehensive Gynecology and Obstetrics) Mikio Mikami - Surgery For Gynecologic Cancer-Springer Singapore (2019)Bakar Benk100% (2)
- Health Unit Plan Disease UnitDocument68 pagesHealth Unit Plan Disease UnitKelly0% (1)
- Emanuel Revici Part 11Document25 pagesEmanuel Revici Part 11db1970No ratings yet
- DR SARMA'S DERMPATH: Chondroma Cutis, The Internet Journal of Dermatology 2007: Volume 6 NumberDocument3 pagesDR SARMA'S DERMPATH: Chondroma Cutis, The Internet Journal of Dermatology 2007: Volume 6 NumberDeba P SarmaNo ratings yet
- M 45, Neck, Asymptomatic Dermal Nodule: Deba P Sarma, MD OmahaDocument4 pagesM 45, Neck, Asymptomatic Dermal Nodule: Deba P Sarma, MD OmahaDeba P SarmaNo ratings yet
- 49 Hemalatha EtalDocument3 pages49 Hemalatha EtaleditorijmrhsNo ratings yet
- Publications 011Document4 pagesPublications 011utamiNo ratings yet
- Solid - Cystic Hidradenoma: A Case ReportDocument5 pagesSolid - Cystic Hidradenoma: A Case ReportIOSRjournalNo ratings yet
- Malignant Myopericytoma: Report of A New Case and Review of The LiteratureDocument6 pagesMalignant Myopericytoma: Report of A New Case and Review of The LiteratureRachel AutranNo ratings yet
- Cerebellopontine Angle Epidermoid CYST: Case ReportDocument3 pagesCerebellopontine Angle Epidermoid CYST: Case ReportTamajyoti GhoshNo ratings yet
- Desdierencia Entre TFS y Glandula ParotidaDocument7 pagesDesdierencia Entre TFS y Glandula ParotidaReyes Ivan García CuevasNo ratings yet
- Rabdomyosarcoma Case ReportDocument7 pagesRabdomyosarcoma Case ReportAaslesha Jakkampudi100% (1)
- Apocrine Mixed TumorDocument5 pagesApocrine Mixed TumorFaduahSalazarNo ratings yet
- Dermatomyofibroma: A Case Report and Review of The LiteratureDocument4 pagesDermatomyofibroma: A Case Report and Review of The LiteratureDeba P SarmaNo ratings yet
- Epidemiological Trends in Malignant Lacrimal Gland TumorsDocument5 pagesEpidemiological Trends in Malignant Lacrimal Gland TumorsRochnald PigaiNo ratings yet
- Benign Extrapleural Solitary Fibrous Tumorofthe Headand NeckDocument7 pagesBenign Extrapleural Solitary Fibrous Tumorofthe Headand NeckCara Danielle PabellanoNo ratings yet
- Articulo de Serie de CasoDocument8 pagesArticulo de Serie de CasoJairo Lino BNo ratings yet
- (12204749 - Romanian Journal of Internal Medicine) Multiple Histological Subtypes of Dermatofibrosarcoma Protuberans Occurring in The Same TumorDocument10 pages(12204749 - Romanian Journal of Internal Medicine) Multiple Histological Subtypes of Dermatofibrosarcoma Protuberans Occurring in The Same TumordrelvNo ratings yet
- Small Round Cells of Head and NeckDocument10 pagesSmall Round Cells of Head and NeckBlazxy EyreNo ratings yet
- Posterior Auricular Mass: Interesting Case SeriesDocument5 pagesPosterior Auricular Mass: Interesting Case SeriesMaria EsterNo ratings yet
- Pilo Matri Coma PosterDocument1 pagePilo Matri Coma Posterkjv5gxdw4fNo ratings yet
- E - Uniform Round Tumour Cells With Small Nucleus and Clear Vacuolated CytoplasmDocument16 pagesE - Uniform Round Tumour Cells With Small Nucleus and Clear Vacuolated CytoplasmAien LeeNo ratings yet
- UC Davis: Dermatology Online JournalDocument4 pagesUC Davis: Dermatology Online Journalma hNo ratings yet
- MTT LabialDocument3 pagesMTT LabialRobertoNo ratings yet
- Adenomyoepithelioma of The Breast: A Brief Diagnostic ReviewDocument5 pagesAdenomyoepithelioma of The Breast: A Brief Diagnostic ReviewSFCHIKINo ratings yet
- Desmoplastic MelanomaDocument3 pagesDesmoplastic MelanomamakhanmdNo ratings yet
- Syringoma 3Document2 pagesSyringoma 3Anita PermatasariNo ratings yet
- Pediatric Desmoid Fibromatosis of TheDocument4 pagesPediatric Desmoid Fibromatosis of ThevatankhahpooyaNo ratings yet
- Pleomorphic Sarcoma in Paratesticular Region: Case Report Open AccessDocument5 pagesPleomorphic Sarcoma in Paratesticular Region: Case Report Open AccessNurulDiniaPutriNo ratings yet
- 1 Ijdrdjun20191Document4 pages1 Ijdrdjun20191TJPRC PublicationsNo ratings yet
- ENGLISH REFARAT 3.2 - Sem 5 - Septina - Malignant Tumours With Follicular DifferentiationDocument28 pagesENGLISH REFARAT 3.2 - Sem 5 - Septina - Malignant Tumours With Follicular DifferentiationAffan Akbar TalamiNo ratings yet
- Keywords: Pilomatrixoma, Skin Nodule, Fine Needle Aspiration CytologyDocument4 pagesKeywords: Pilomatrixoma, Skin Nodule, Fine Needle Aspiration CytologyachmadaNo ratings yet
- Basal Cell AdenomawDocument3 pagesBasal Cell AdenomawDrRobin SabharwalNo ratings yet
- Ameloblastoma: Notorious Tumor of The Jaw - Report of A CaseDocument3 pagesAmeloblastoma: Notorious Tumor of The Jaw - Report of A CaseUwie MoumootNo ratings yet
- Dermatology Research and Therapy: Nodular Hidradenoma: A Forgotten Tumor of The ScalpDocument3 pagesDermatology Research and Therapy: Nodular Hidradenoma: A Forgotten Tumor of The ScalpannibaNo ratings yet
- Ijohns 2015083115062935 PDFDocument6 pagesIjohns 2015083115062935 PDFradifNo ratings yet
- Chondrosarcoma of Breast - A Case ReportDocument2 pagesChondrosarcoma of Breast - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- RPB14150079015Document5 pagesRPB14150079015Ijupbs IjupbsNo ratings yet
- 1868-Article Text-6804-1-10-20180620Document3 pages1868-Article Text-6804-1-10-20180620Wina ViqaNo ratings yet
- Oligodendroglioma in The Cervical Spinal Cord of A Dog: T. M, A. M - L, M. H - T, W. BDocument3 pagesOligodendroglioma in The Cervical Spinal Cord of A Dog: T. M, A. M - L, M. H - T, W. BSamir BazanNo ratings yet
- Plastic Surgery & Advanced Scalp Tumors: Epidemiological Profile and Surgical Management About 65 CasesDocument7 pagesPlastic Surgery & Advanced Scalp Tumors: Epidemiological Profile and Surgical Management About 65 CasesIJAR JOURNALNo ratings yet
- Additional Article Information: Keywords: Adenoid Cystic Carcinoma, Cribriform Pattern, Parotid GlandDocument7 pagesAdditional Article Information: Keywords: Adenoid Cystic Carcinoma, Cribriform Pattern, Parotid GlandRizal TabootiNo ratings yet
- Laryngeal Plasmacytoma in Kahlers Disease: A Case ReportDocument6 pagesLaryngeal Plasmacytoma in Kahlers Disease: A Case ReportIJAR JOURNALNo ratings yet
- Adenoid Cystic Carcinoma of Hard Palate: A Case ReportDocument5 pagesAdenoid Cystic Carcinoma of Hard Palate: A Case ReportHemant GuptaNo ratings yet
- Case Report Reference Article (Published)Document3 pagesCase Report Reference Article (Published)manojananthappanNo ratings yet
- Metaplastic Carcinoma Breast: A Case SeriesDocument4 pagesMetaplastic Carcinoma Breast: A Case SeriesIJAR JOURNALNo ratings yet
- Adult LymphangiomaDocument3 pagesAdult LymphangiomaRini RahmawulandariNo ratings yet
- A Rare Case of Zosteriform Cutaneous Metastasesfrom Squamous Cell Carcinoma of Hard PalateDocument4 pagesA Rare Case of Zosteriform Cutaneous Metastasesfrom Squamous Cell Carcinoma of Hard PalateShiva PNo ratings yet
- 45syam EtalDocument3 pages45syam EtaleditorijmrhsNo ratings yet
- Article - Cytological Features of The Warthin-Like Variant of Salivary Mucoepidermoid CarcinomaDocument5 pagesArticle - Cytological Features of The Warthin-Like Variant of Salivary Mucoepidermoid CarcinomaCandeNo ratings yet
- Hasil Penelitian KSSDocument3 pagesHasil Penelitian KSSMarlboro LightsNo ratings yet
- Abstract: Kimura Disease Is A Rare Form of Chronic Inflammatory Disorder InvolvingDocument4 pagesAbstract: Kimura Disease Is A Rare Form of Chronic Inflammatory Disorder InvolvingpriyokNo ratings yet
- CH15 Patho D&R AgamDocument11 pagesCH15 Patho D&R AgamBio CheNo ratings yet
- 8veda EtalDocument7 pages8veda EtaleditorijmrhsNo ratings yet
- Case Report Epithelial-Myoepithelial Carcinoma of The Breast With Rhabdoid FeaturesDocument4 pagesCase Report Epithelial-Myoepithelial Carcinoma of The Breast With Rhabdoid FeaturesGabriela Izabela BaltatescuNo ratings yet
- Melanome Acral: Du Diagnostic Au TraitementDocument8 pagesMelanome Acral: Du Diagnostic Au TraitementIJAR JOURNALNo ratings yet
- A Case Report of Eruptive Syringoma: Clinical, Dermoscopic and Histological FeaturesDocument5 pagesA Case Report of Eruptive Syringoma: Clinical, Dermoscopic and Histological FeaturesIJAR JOURNALNo ratings yet
- ContentsDocument3 pagesContentsNaim CalilNo ratings yet
- 18 Extra-GuptaNDocument3 pages18 Extra-GuptaNGalih rarang gatiNo ratings yet
- Current Controversies in The Management of Malignant Parotid TumorsDocument8 pagesCurrent Controversies in The Management of Malignant Parotid TumorsDirga Rasyidin LNo ratings yet
- Low Grade Endometrial Stromal Sarcoma: A Case ReportDocument3 pagesLow Grade Endometrial Stromal Sarcoma: A Case ReportNazia BhatNo ratings yet
- 03.04 - Intraventricular TumoursDocument185 pages03.04 - Intraventricular TumoursBivolaru AlinNo ratings yet
- Basal Cell Carcinoma: Advances in Treatment and ResearchFrom EverandBasal Cell Carcinoma: Advances in Treatment and ResearchMichael R. MigdenNo ratings yet
- Accessory TragusDocument3 pagesAccessory TragusDeba P SarmaNo ratings yet
- Acantholytic Dermatosis With DyskeratosisDocument11 pagesAcantholytic Dermatosis With DyskeratosisDeba P SarmaNo ratings yet
- Pilar Cyst With CrystalsDocument2 pagesPilar Cyst With CrystalsDeba P SarmaNo ratings yet
- Acantholytic Solar Keratosis, M 67, Forehead PDFDocument6 pagesAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNo ratings yet
- Acantholytic Bullous DiseaseDocument4 pagesAcantholytic Bullous DiseaseDeba P SarmaNo ratings yet
- Acantholytic Actinic KeratosisDocument4 pagesAcantholytic Actinic KeratosisDeba P SarmaNo ratings yet
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Document3 pagesAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNo ratings yet
- Xanthogranuloma PPT DSDocument9 pagesXanthogranuloma PPT DSDeba P SarmaNo ratings yet
- Acantholytic Acanthoma. M 60, ScrotumDocument8 pagesAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNo ratings yet
- Results of Search in Google Scholar On 'Deba P Sarma'Document28 pagesResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNo ratings yet
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Document6 pagesBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNo ratings yet
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDocument7 pagesXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNo ratings yet
- Xanthogranuloma, M 30, Right ElbowDocument4 pagesXanthogranuloma, M 30, Right ElbowDeba P SarmaNo ratings yet
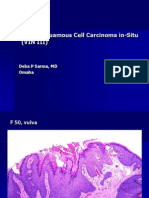
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDocument6 pagesVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNo ratings yet
- Verrucous Epidermal Nevus. F 43, ScalpDocument4 pagesVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNo ratings yet
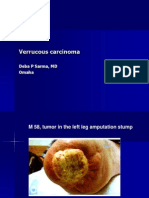
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDocument7 pagesVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNo ratings yet
- Verrucous Carcinoma of The Foot, M 63, Left FootDocument8 pagesVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Verruca Vulgaris., M 22.,PPTDocument2 pagesVerruca Vulgaris., M 22.,PPTDeba P SarmaNo ratings yet
- Jurnal Autoimun PDFDocument7 pagesJurnal Autoimun PDFRara Anglis AninditaNo ratings yet
- Agenda - Biblioteka de Biomarkeri - FINALDocument1 pageAgenda - Biblioteka de Biomarkeri - FINALOlteanu Gheorghe-EmilianNo ratings yet
- Combating Lifestyle Diseases in Kerala With Ayurvedic RegimenDocument6 pagesCombating Lifestyle Diseases in Kerala With Ayurvedic RegimenarcherselevatorsNo ratings yet
- Cap. 1 PDFDocument44 pagesCap. 1 PDFOscarNo ratings yet
- Tumori Fibrohistiocitare IntermediareDocument39 pagesTumori Fibrohistiocitare IntermediareOana BarbuNo ratings yet
- Survivor Stories: Living With, Through & Beyond CancerDocument24 pagesSurvivor Stories: Living With, Through & Beyond CancerTedEscobedoNo ratings yet
- USPSTF Screening Recommendations (Across The Ages)Document8 pagesUSPSTF Screening Recommendations (Across The Ages)Jessica MooreNo ratings yet
- Cell Division - Mitosis and The Cell CycleDocument43 pagesCell Division - Mitosis and The Cell CycleJomar CarabotNo ratings yet
- Cordyceps Militaris CapsuleDocument32 pagesCordyceps Militaris CapsuleDeborah o100% (1)
- Nejmoa1113162 AppendixDocument35 pagesNejmoa1113162 AppendixayuannisahusnaNo ratings yet
- Chapter 5 - Autosuggestion - Think and Grow Rich - The 21st-Century Edition (Workbook)Document33 pagesChapter 5 - Autosuggestion - Think and Grow Rich - The 21st-Century Edition (Workbook)Naveed AhmedNo ratings yet
- Kep KritisDocument193 pagesKep Kritisari cahyaNo ratings yet
- Optic Nerve Tumours: Presenter-Dr Adheela Abdulla Moderator - DR Shikha BassiDocument54 pagesOptic Nerve Tumours: Presenter-Dr Adheela Abdulla Moderator - DR Shikha BassiMohammed Jazeel 2549No ratings yet
- Pharmaceutical Probability of SuccessDocument42 pagesPharmaceutical Probability of SuccesskennyNo ratings yet
- Elective Clinical Target Volumes For Conformal Therapy in Anorectal Cancer - An Radiation Therapy Oncology Group Consensus Panel Contouring AtlasDocument7 pagesElective Clinical Target Volumes For Conformal Therapy in Anorectal Cancer - An Radiation Therapy Oncology Group Consensus Panel Contouring AtlasAnonymous 8KN8IR1GTWNo ratings yet
- Nutrition Assessment 1Document22 pagesNutrition Assessment 1KHALEEL SALEHNo ratings yet
- 10 1 Paraneoplastic SyndromesDocument31 pages10 1 Paraneoplastic SyndromesTeky WidyariniNo ratings yet
- Care of Clients With Problems in Cellular Aberrations Key TermsDocument2 pagesCare of Clients With Problems in Cellular Aberrations Key Termsjoyrena ochondraNo ratings yet
- Basic Oncology RadiationDocument30 pagesBasic Oncology Radiationnugra raturandangNo ratings yet
- 28 11 2019 8th Aitong Medical Camp ReportDocument26 pages28 11 2019 8th Aitong Medical Camp ReportStacy NeetNo ratings yet
- Top 10 Healthiest FruitDocument15 pagesTop 10 Healthiest FruitFauzia IkaNo ratings yet
- Cancer - 2011 - Hajdu - A Note From History Landmarks in History of Cancer Part 2Document10 pagesCancer - 2011 - Hajdu - A Note From History Landmarks in History of Cancer Part 2Pilar AufrastoNo ratings yet
- CPH LEC (05-05) - Unit 4Document4 pagesCPH LEC (05-05) - Unit 4Ruthenie RedobleNo ratings yet
- HPV QUANT-21 - Form A6 - Specification of ProductDocument4 pagesHPV QUANT-21 - Form A6 - Specification of ProductLAB PCRNo ratings yet
- Pyrexia of Unknown OriginDocument81 pagesPyrexia of Unknown OriginJithin Bhagavati Kalam100% (1)
- End of Term 3 Musomhs Cat MCQ July 2020-1Document16 pagesEnd of Term 3 Musomhs Cat MCQ July 2020-1MustafaNo ratings yet