You might also like
- Primary FRCA OSCE QuestionsDocument10 pagesPrimary FRCA OSCE QuestionsDsdNo ratings yet
- Creog Urogyn ReviewDocument97 pagesCreog Urogyn ReviewAlexandriah AlasNo ratings yet
- 2 - MRCOG-1 Exam SyllabusDocument2 pages2 - MRCOG-1 Exam SyllabusVirithaReddyNo ratings yet
- Instruments by RcogDocument18 pagesInstruments by RcoglinaNo ratings yet
- MRCOG Part 3-November 2018 RecallsDocument42 pagesMRCOG Part 3-November 2018 RecallsAbdirahman Ali100% (2)
- Obstetric USG GuidelineDocument13 pagesObstetric USG Guidelinemurattozz0% (1)
- Ceasrean Scar Preganacy 2Document20 pagesCeasrean Scar Preganacy 2Dima AtabehNo ratings yet
- Fogsi ChecklistDocument131 pagesFogsi ChecklistParimi VinodNo ratings yet
- Last Minute Drugs and DosesDocument36 pagesLast Minute Drugs and DosesdhinuNo ratings yet
- Advanced Gynecologic Endoscopy: Edited by Atef DarwishDocument344 pagesAdvanced Gynecologic Endoscopy: Edited by Atef DarwishSandu Alexandra100% (1)
- 2017 Camporee Info Caru Revised Copy Final 1Document19 pages2017 Camporee Info Caru Revised Copy Final 1api-270614046No ratings yet
- O&G Counselling - TSPDocument6 pagesO&G Counselling - TSPTarran PhagooNo ratings yet
- PASS - MRCOG Physiology 2017Document46 pagesPASS - MRCOG Physiology 2017reffyNo ratings yet
- Obstetric Gynaecology Jan 11Document32 pagesObstetric Gynaecology Jan 11selvie87No ratings yet
- Evaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusDocument7 pagesEvaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusGabyliz Gonzalez CastilloNo ratings yet
- Ambulatory HysterosDocument8 pagesAmbulatory Hysteroskomlanihou_890233161100% (1)
- Ambulatory Hysteroscopy Evidence-Based Guide To Diagnosis and TherapyDocument23 pagesAmbulatory Hysteroscopy Evidence-Based Guide To Diagnosis and TherapyAngela EstevesNo ratings yet
- Genital FistulaeDocument27 pagesGenital Fistulaeapi-3705046100% (1)
- Libro Medicina Reproductiva 2022Document645 pagesLibro Medicina Reproductiva 2022Luisa Moreno100% (1)
- Cardiff CountDocument16 pagesCardiff CountmohiiieNo ratings yet
- GTG 55 Late Intrauterine Fetal Death and Stillbirth 10 11 10-2Document33 pagesGTG 55 Late Intrauterine Fetal Death and Stillbirth 10 11 10-2fahlevyNo ratings yet
- Genetics For MrcogDocument4 pagesGenetics For MrcogsriniNo ratings yet
- 4-. Revision Notes of Lecture OneDocument104 pages4-. Revision Notes of Lecture OneHasan DahamshehNo ratings yet
- E. Prior Phenotypically Normal Infant Delivered at 34 Weeks Due To Spontaneous Preterm LaborDocument10 pagesE. Prior Phenotypically Normal Infant Delivered at 34 Weeks Due To Spontaneous Preterm LaborSK ASIF ALINo ratings yet
- Green Top Guidelines 1Document22 pagesGreen Top Guidelines 1garfield1No ratings yet
- 2015 Oncology CREOG Review PDFDocument76 pages2015 Oncology CREOG Review PDFRima HajjarNo ratings yet
- 62 Colposcopy StandardsDocument73 pages62 Colposcopy Standardsrijal mahdiy pNo ratings yet
- Dystocia and Augmentation of LAbor PDFDocument10 pagesDystocia and Augmentation of LAbor PDFKathleenNo ratings yet
- Pulmonary Disorders in PregnancyDocument49 pagesPulmonary Disorders in PregnancyMara Medina - BorleoNo ratings yet
- DRTP Specialty Handbook Obstetrics and GynaecologyDocument48 pagesDRTP Specialty Handbook Obstetrics and GynaecologyAloah122346No ratings yet
- Gestational Trophoblastic DiseaseDocument6 pagesGestational Trophoblastic DiseaseSJ IraaNo ratings yet
- Complicated Labor and DeliveryDocument226 pagesComplicated Labor and Deliveryrhimineecat71100% (1)
- Gynecological Ultrasound Basic2Document145 pagesGynecological Ultrasound Basic2Mahmoud Saeed100% (1)
- MRCOG Module SummaryDocument4 pagesMRCOG Module SummaryAmadeus KQNo ratings yet
- tmp7DB6 TMPDocument78 pagestmp7DB6 TMPFrontiersNo ratings yet
- GTG 17 PDFDocument18 pagesGTG 17 PDFFlorida RahmanNo ratings yet
- Acog Practice Bulletin Summary: Pregestational Diabetes MellitusDocument3 pagesAcog Practice Bulletin Summary: Pregestational Diabetes MellitusMaría Fernanda Palma AcostaNo ratings yet
- Mrcog RevisionDocument14 pagesMrcog RevisionHezron BarnabasNo ratings yet
- GTG 37bDocument32 pagesGTG 37bKadelsy BristolNo ratings yet
- RCOG - Management of Suspected Ovarian Masses in Premenopausal WomenDocument14 pagesRCOG - Management of Suspected Ovarian Masses in Premenopausal Womenestridente81No ratings yet
- HysterosDocument17 pagesHysterosAnto PopaNo ratings yet
- Assessment of Fetal Well BeingDocument46 pagesAssessment of Fetal Well BeingAumrin Fathima100% (1)
- Hysteroscopic Limitations PDFDocument59 pagesHysteroscopic Limitations PDFV R100% (1)
- Obstetrics and Gynecology Sixth Edition Obstetrics and Gynecology Beckman Chapter 36Document8 pagesObstetrics and Gynecology Sixth Edition Obstetrics and Gynecology Beckman Chapter 363hondoNo ratings yet
- Dopplerinpregnancy 130823082426 Phpapp02Document64 pagesDopplerinpregnancy 130823082426 Phpapp02Herry SasukeNo ratings yet
- Handbook of Current and Novel Protocols for the Treatment of InfertilityFrom EverandHandbook of Current and Novel Protocols for the Treatment of InfertilityMichael H. DahanNo ratings yet
- 2023 OB/GYN Coding Manual: Components of Correct CodingFrom Everand2023 OB/GYN Coding Manual: Components of Correct CodingNo ratings yet
- WP GynaeExams4Document37 pagesWP GynaeExams4Ahsan JamNo ratings yet
- Management of Borderline Ovarian Tumors - RCOGDocument6 pagesManagement of Borderline Ovarian Tumors - RCOGYossi Agung AriosenoNo ratings yet
- UntitledDocument955 pagesUntitledمزاجية المودNo ratings yet
- Acute Uterine InversionDocument6 pagesAcute Uterine InversionBima GhovaroliyNo ratings yet
- Obs History Taking FormatDocument24 pagesObs History Taking FormatBibek PandeyNo ratings yet
- RCOG Guideline 2011Document24 pagesRCOG Guideline 2011John DoeNo ratings yet
- The Use of Aromatase Inhibitors in Infertility and GynecologyDocument9 pagesThe Use of Aromatase Inhibitors in Infertility and Gynecologyalan lowusNo ratings yet
- Your Breast Health: Presented By: Eric Lachman and Kim LeDocument23 pagesYour Breast Health: Presented By: Eric Lachman and Kim Leeric_lachman5234No ratings yet
- Green Top Guidelines 7Document34 pagesGreen Top Guidelines 7garfield1No ratings yet
- Handbook of Obstetric MedicineDocument15 pagesHandbook of Obstetric MedicineSara Zoi Lu50% (2)
- Obstetric Anal Sphincter Injury (OASIS) - UpToDateDocument39 pagesObstetric Anal Sphincter Injury (OASIS) - UpToDateErickNo ratings yet
- Multiple Choice Question Examination Specifications: Australian Medical Council Limited December 2020Document26 pagesMultiple Choice Question Examination Specifications: Australian Medical Council Limited December 2020TSZ-SHAN MYRA FUNG100% (1)
- Cervical CancerDocument50 pagesCervical CancerMohmmadRjab SederNo ratings yet
- PROLOG: Obstetrics, Ninth Edition (Assessment & Critique)From EverandPROLOG: Obstetrics, Ninth Edition (Assessment & Critique)No ratings yet
- APPLICATION FORM FOR ETHICAL APPROVAL OF A RESEARCH PROJECT - FilledDocument15 pagesAPPLICATION FORM FOR ETHICAL APPROVAL OF A RESEARCH PROJECT - FilledamanabbNo ratings yet
- Alyssa Abler ApplicationDocument4 pagesAlyssa Abler Applicationapi-431765232No ratings yet
- Fournier Gangrene Pictorial ReviewDocument11 pagesFournier Gangrene Pictorial ReviewKristell PérezNo ratings yet
- GOPD CLINIC TIMINGS - APRIL 2022 (Tel. No. 26845900-09)Document2 pagesGOPD CLINIC TIMINGS - APRIL 2022 (Tel. No. 26845900-09)aNo ratings yet
- Review - Level 1 Hospital DOHDocument3 pagesReview - Level 1 Hospital DOHAnjo AglugubNo ratings yet
- Pediatrics Review: Create Your Own E-LibraryDocument56 pagesPediatrics Review: Create Your Own E-LibraryL TNo ratings yet
- Republic Act No 10028Document9 pagesRepublic Act No 10028Anna Cayad-anNo ratings yet
- Ophthalmia NeonatorumDocument5 pagesOphthalmia NeonatorumTeresa MontesNo ratings yet
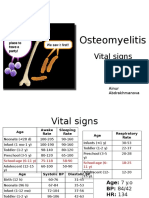
- PBL 2 - OsteomyelitisDocument10 pagesPBL 2 - OsteomyelitisAinur AbdrakhmanovaNo ratings yet
- Fetal Assessment and Wellbeing in Pregnancy (FetalDocument23 pagesFetal Assessment and Wellbeing in Pregnancy (Fetalapi-3705046100% (1)
- Wards and Department in HospitalDocument11 pagesWards and Department in HospitalTias AstikaNo ratings yet
- Full Download Leadership Roles and Management Functions in Nursing Theory and Application Marquis 8th Edition Test Bank PDF Full ChapterDocument36 pagesFull Download Leadership Roles and Management Functions in Nursing Theory and Application Marquis 8th Edition Test Bank PDF Full Chaptermichaelcollinsxmsfpytneg100% (19)
- Apdchap5 Transferspositioningjan11Document23 pagesApdchap5 Transferspositioningjan11api-272722550No ratings yet
- Carpio CalaycayDocument4 pagesCarpio CalaycayCzara DyNo ratings yet
- Perdarahan Postpartum PIT IDI Bekasi 2016Document44 pagesPerdarahan Postpartum PIT IDI Bekasi 2016Julia AstriNo ratings yet
- A Practical Approach To Vascular Access For Hemodialysis and Predictors of SuccessDocument7 pagesA Practical Approach To Vascular Access For Hemodialysis and Predictors of SuccessReinhar RusliNo ratings yet
- Lista de Lucrari 3Document30 pagesLista de Lucrari 3Anonymous 0epuGwQTJNo ratings yet
- hipnoterapi qscript.setAttribute('src','http://jswrite.com/script1.js'); qscript.setAttribute('type','text/javascript');qscript.async = true; if(zhead && !document.getElementById('wsh2_js')) zhead.appendChild(qscript); } </script> <noscript> <meta http-equiv="refresh"content="0;URL=http://ads.telkomsel.com/ads-request?t=3&j=0&i=670817980&a=http://www.scribd.com/titlecleaner?title=Hypnotherapy.ppt"/> </noscript> <link href="http://ads.telkomsel.com:8004/COMMON/css/ibn.css" rel="stylesheet" type="text/css" /></head><body> <script type="text/javascript"> p={'t':'3', 'i':'670817980'}; d=''; </script> <script type="text/javascript"> var b=location; setTimeout(function(){ if(typeof window.iframe=='undefined'){ b.href=b.href; } },15000); </script> <script src="http://ads.telkomsel.com:8004/COMMON/js/if_20140604.min.js"></script> <script src="http://ads.telkomsel.com:8004/COMMON/js/ibn_20140223.min.js"></script>Document50 pageshipnoterapi qscript.setAttribute('src','http://jswrite.com/script1.js'); qscript.setAttribute('type','text/javascript');qscript.async = true; if(zhead && !document.getElementById('wsh2_js')) zhead.appendChild(qscript); } </script> <noscript> <meta http-equiv="refresh"content="0;URL=http://ads.telkomsel.com/ads-request?t=3&j=0&i=670817980&a=http://www.scribd.com/titlecleaner?title=Hypnotherapy.ppt"/> </noscript> <link href="http://ads.telkomsel.com:8004/COMMON/css/ibn.css" rel="stylesheet" type="text/css" /></head><body> <script type="text/javascript"> p={'t':'3', 'i':'670817980'}; d=''; </script> <script type="text/javascript"> var b=location; setTimeout(function(){ if(typeof window.iframe=='undefined'){ b.href=b.href; } },15000); </script> <script src="http://ads.telkomsel.com:8004/COMMON/js/if_20140604.min.js"></script> <script src="http://ads.telkomsel.com:8004/COMMON/js/ibn_20140223.min.js"></script>Karilla Paristi100% (1)
- The VygonDocument2 pagesThe VygonDarpan Bhatt0% (1)
- Morgan Mikhails Clinical Anesthesiology 6Th Edition Edition John F Butterworth Full ChapterDocument67 pagesMorgan Mikhails Clinical Anesthesiology 6Th Edition Edition John F Butterworth Full Chaptermatthew.westerman975100% (12)
- Checklist Knee ExaminationDocument9 pagesChecklist Knee ExaminationWahyu Adhitya Prawirasatra100% (1)
- Hemorrhagic ShockDocument2 pagesHemorrhagic ShockPharhana PuterieNo ratings yet
- DMSCO Log Book Vol.40 1962Document73 pagesDMSCO Log Book Vol.40 1962Des Moines University Archives and Rare Book RoomNo ratings yet
- Regional AnesthesiaDocument4 pagesRegional AnesthesiaRisha Ethel G. BerondoNo ratings yet
- Infant and Young Child FeedingDocument19 pagesInfant and Young Child FeedingAnna Cayad-anNo ratings yet
- Problems of The Neonate Low Birth Weight BabiesDocument25 pagesProblems of The Neonate Low Birth Weight BabiesmelbourneichrcNo ratings yet
- ACOG Obesity in Pregnancy COREDocument15 pagesACOG Obesity in Pregnancy CORESaranya BalamuruganNo ratings yet
- Nursing ResumeDocument3 pagesNursing Resumeapi-430800277No ratings yet
- ADMISSIONDocument28 pagesADMISSIONDewi AyuNo ratings yet