You might also like
- Temporal Bone Imaging: Comparison of Flat Panel Volume CT and Multisection CTDocument6 pagesTemporal Bone Imaging: Comparison of Flat Panel Volume CT and Multisection CTNovi DwiyantiNo ratings yet
- CT SacnDocument6 pagesCT SacnmartinNo ratings yet
- Wall TrackingDocument14 pagesWall TrackinghoplalaNo ratings yet
- Absorbed Dose in Mgy From CT ScannersDocument9 pagesAbsorbed Dose in Mgy From CT Scannerscebuano88No ratings yet
- 3D cone-beam CT of the ankle using a novel twin robotic X-ray systemDocument7 pages3D cone-beam CT of the ankle using a novel twin robotic X-ray systemanderson.mancianoNo ratings yet
- Hyer2010xvi DoseDocument17 pagesHyer2010xvi DoseÖzgür Kara (OncoHealth)No ratings yet
- Development and Validation of A Low Dose Simulation Algorithm For Computed TomographyDocument9 pagesDevelopment and Validation of A Low Dose Simulation Algorithm For Computed TomographyBrankica MitrovicNo ratings yet
- Ut FractalDocument5 pagesUt FractalDemian PereiraNo ratings yet
- Characterization and evaluation of 2.5 MV electronic portal imaging for accurate localization of intra- and extracranial stereotactic radiosurgeryDocument17 pagesCharacterization and evaluation of 2.5 MV electronic portal imaging for accurate localization of intra- and extracranial stereotactic radiosurgeryzhen yongjieNo ratings yet
- 1 s2.0 S2212440312000442 MainDocument6 pages1 s2.0 S2212440312000442 MainMarinaNo ratings yet
- Real-Time Spatial Compound ImagingDocument2 pagesReal-Time Spatial Compound ImagingNam LeNo ratings yet
- Radiation Dose in Pelvic ImagingDocument9 pagesRadiation Dose in Pelvic ImagingAlmvd DelgadoNo ratings yet
- Image Quality Comparison of IGRT DevicesDocument7 pagesImage Quality Comparison of IGRT Devicesface bookNo ratings yet
- TAC PeñascoDocument10 pagesTAC PeñascoJose ManuelNo ratings yet
- Sicotj 8 34Document5 pagesSicotj 8 34robertoNo ratings yet
- Qims 12 01 766Document15 pagesQims 12 01 766Hamza ArjahNo ratings yet
- Medical Physics - 2021 - Praagh - Fully Automated Quantification Method FQM of Coronary Calcium in An AnthropomorphicDocument12 pagesMedical Physics - 2021 - Praagh - Fully Automated Quantification Method FQM of Coronary Calcium in An AnthropomorphicAmril MukminNo ratings yet
- Ijri 29 53Document8 pagesIjri 29 53Kelum BuddhikaNo ratings yet
- Chan 2015Document10 pagesChan 2015Innes AndrianiNo ratings yet
- Resume C-ArmDocument4 pagesResume C-Armp27838121011No ratings yet
- A New Method of MRI Examination For The Sternoclavicular JointsDocument12 pagesA New Method of MRI Examination For The Sternoclavicular JointsRafael CamposNo ratings yet
- PHY321GE2 Medical Imaging PDFDocument19 pagesPHY321GE2 Medical Imaging PDFPathmathasNo ratings yet
- Ghid Plex Brahial Conturaj PDFDocument7 pagesGhid Plex Brahial Conturaj PDFMiruna MafteiNo ratings yet
- Literature Review of Uwb AntennaDocument7 pagesLiterature Review of Uwb Antennac5ppm3e3100% (1)
- Cal Dose X ManualDocument23 pagesCal Dose X ManualRadiologi RSUD CiawiNo ratings yet
- LN3Document6 pagesLN3Haseeb QuadriNo ratings yet
- J Applied Clin Med Phys - 2016 - Dodge - Performance Evaluation of Iterative Reconstruction Algorithms For Achieving CTDocument22 pagesJ Applied Clin Med Phys - 2016 - Dodge - Performance Evaluation of Iterative Reconstruction Algorithms For Achieving CTAmril MukminNo ratings yet
- Basic Principles and Technical Considerations: Radiographic AbsorptiometryDocument10 pagesBasic Principles and Technical Considerations: Radiographic AbsorptiometrySatria Adi PutraNo ratings yet
- Denoising of Contrast-Enhanced Ultrasound Cine Sequences Based On A Multiplicative ModelDocument12 pagesDenoising of Contrast-Enhanced Ultrasound Cine Sequences Based On A Multiplicative ModelKarthick VijayanNo ratings yet
- Computerized Detection of Lung Nodules by Means of "Virtual Dual-Energy" RadiographyDocument10 pagesComputerized Detection of Lung Nodules by Means of "Virtual Dual-Energy" RadiographyAntony RatheeshNo ratings yet
- Exposure Chart Mobile X Ray PDFDocument8 pagesExposure Chart Mobile X Ray PDFlutfiaNo ratings yet
- Diagnostic Aids in OrthodonticsDocument12 pagesDiagnostic Aids in OrthodonticsNevin Abraham100% (1)
- Analysis of The Accuracy of Linear Measurements Obtained by Cone Beam Computed Tomography (Cbct-Newtom)Document4 pagesAnalysis of The Accuracy of Linear Measurements Obtained by Cone Beam Computed Tomography (Cbct-Newtom)BalwantNo ratings yet
- Multiparametric Whole Body MRI With Diffusion Weighted Imaging - 2018 - AcademiDocument10 pagesMultiparametric Whole Body MRI With Diffusion Weighted Imaging - 2018 - AcademiRicardo MirandaNo ratings yet
- Alacam2008 2 2Document23 pagesAlacam2008 2 2John JonesNo ratings yet
- Organ and Effective Dose Reduction in Adult Chest CT UsingDocument7 pagesOrgan and Effective Dose Reduction in Adult Chest CT UsingIshani Anushika JayakodyNo ratings yet
- Radiation Dose Reduction Techniques For Chest CT Principles and Clinical ResultsDocument11 pagesRadiation Dose Reduction Techniques For Chest CT Principles and Clinical ResultsSantiago TapiaNo ratings yet
- A Simulation-Based Assessment of The Revised NEMA NU-2 70-cm Long Test Phantom For PETDocument5 pagesA Simulation-Based Assessment of The Revised NEMA NU-2 70-cm Long Test Phantom For PETMarcelo ToledoNo ratings yet
- J Applied Clin Med Phys - 2023 - Ikeda - Impact of CT Scan Parameters On Deformable Image Registration Accuracy UsingDocument9 pagesJ Applied Clin Med Phys - 2023 - Ikeda - Impact of CT Scan Parameters On Deformable Image Registration Accuracy UsingPiotr JankowskiNo ratings yet
- Detective Quantum Efficiency Measured As A Function of Energy For Two Full-Field Digital Mammography SystemsDocument18 pagesDetective Quantum Efficiency Measured As A Function of Energy For Two Full-Field Digital Mammography SystemsAllan Amaral da HoraNo ratings yet
- Dual-Source CT and The Effect of Tin Filtration On ImageDocument6 pagesDual-Source CT and The Effect of Tin Filtration On Imagemas bejo01No ratings yet
- Measuring Limb Length Discrepancy Using Pelvic Radiographs: The Most Reproducible MethodDocument5 pagesMeasuring Limb Length Discrepancy Using Pelvic Radiographs: The Most Reproducible MethodBudhiNo ratings yet
- Ultrasound Machine Research PaperDocument5 pagesUltrasound Machine Research Paperpukytij0wyg3100% (1)
- Radiologic Clinics of North America Body MR Imaging, Volume 41 Number 1 2003Document193 pagesRadiologic Clinics of North America Body MR Imaging, Volume 41 Number 1 2003pepsimax85No ratings yet
- Use of Cone Beam Computed Tomography in EndodonticsDocument67 pagesUse of Cone Beam Computed Tomography in EndodonticsDr.O.R.GANESAMURTHINo ratings yet
- Dose-Reduction Experiment During A Cervical Vertebrae ExaminationDocument12 pagesDose-Reduction Experiment During A Cervical Vertebrae ExaminationDesty ArianiNo ratings yet
- Correlation Between CT Numbers and Tissue Parameters Needed For Monte Carlo Simulations of Clinical Dose DistributionsDocument21 pagesCorrelation Between CT Numbers and Tissue Parameters Needed For Monte Carlo Simulations of Clinical Dose DistributionsMatheus AlvarezNo ratings yet
- Integrated SFCW Transceivers For UWB Breast Cancer Imaging: Architectures and Circuit ConstraintsDocument14 pagesIntegrated SFCW Transceivers For UWB Breast Cancer Imaging: Architectures and Circuit ConstraintsJesus Alejandro Amaya HernandezNo ratings yet
- Shouldconebeam Computedtomographybe Routinelyobtainedinimplant Planning?Document17 pagesShouldconebeam Computedtomographybe Routinelyobtainedinimplant Planning?javiers45No ratings yet
- Volume Computed Tomography Air Kerma Index and Image Quality Evaluation in BrazilDocument5 pagesVolume Computed Tomography Air Kerma Index and Image Quality Evaluation in BrazilAhmed AlkabodyNo ratings yet
- DeformitiesDocument10 pagesDeformitiesNitya KrishnaNo ratings yet
- Full PDFDocument8 pagesFull PDFGabriella LintinNo ratings yet
- Physics and Imaging in Radiation OncologyDocument6 pagesPhysics and Imaging in Radiation Oncologydarr artNo ratings yet
- SimuladasDocument9 pagesSimuladasHENRIQUE AUGUSTO LINONo ratings yet
- Two-Versus Three-Dimensional Imaging in Subjects With Unerupted Maxillary CaninesDocument6 pagesTwo-Versus Three-Dimensional Imaging in Subjects With Unerupted Maxillary CaninesAkram AlsharaeeNo ratings yet
- Assessment PDFDocument7 pagesAssessment PDFdrprasantNo ratings yet
- The Eos ™ Imaging System and Its Uses in Daily Orthopaedic PracticeDocument7 pagesThe Eos ™ Imaging System and Its Uses in Daily Orthopaedic PracticeRoman PopescuNo ratings yet
- The Physics and Technology of Diagnostic Ultrasound: Study Guide (Second Edition)From EverandThe Physics and Technology of Diagnostic Ultrasound: Study Guide (Second Edition)No ratings yet
- Plug-In Gait Model DetailsDocument23 pagesPlug-In Gait Model DetailsElbe MirandaNo ratings yet
- Anatomy AssignDocument25 pagesAnatomy AssignAdarshBijapurNo ratings yet
- Chiropractic Adjusting TechniqueDocument111 pagesChiropractic Adjusting TechniqueDavid CristanchoNo ratings yet
- Static Palpation of The Spine FINALDocument13 pagesStatic Palpation of The Spine FINALPrathap KumarNo ratings yet
- Biomechanics of The Lumbar Spine: Shira Schecter Weiner, Florian Brunner, and Margareta NordinDocument27 pagesBiomechanics of The Lumbar Spine: Shira Schecter Weiner, Florian Brunner, and Margareta NordinpkrajniNo ratings yet
- HBS 2 1 2 PLTWDocument10 pagesHBS 2 1 2 PLTWDECA InquiryNo ratings yet
- 10 Lumbosacral SpineDocument10 pages10 Lumbosacral Spine楊畯凱No ratings yet
- Muscles of The BackDocument33 pagesMuscles of The Backtaha makhloufNo ratings yet
- Anatomy Imporatant Points by Dr. Asif AliDocument31 pagesAnatomy Imporatant Points by Dr. Asif AliSyed imran AbbasNo ratings yet
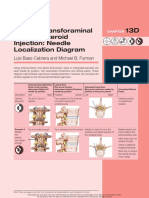
- Lumbar Transforaminal Epidural Steroid Injection: Needle Localization DiagramDocument2 pagesLumbar Transforaminal Epidural Steroid Injection: Needle Localization DiagramSoumabho DasNo ratings yet
- Skull Thoracic Cage (Ribs and Sternum) Facial Bones Cranium: Chapter 7 - The SkeletonDocument45 pagesSkull Thoracic Cage (Ribs and Sternum) Facial Bones Cranium: Chapter 7 - The SkeletonSoua YangNo ratings yet
- (Gregory D. Cramer, Susan A. Darby) Basic and ClinDocument450 pages(Gregory D. Cramer, Susan A. Darby) Basic and ClinAna-Maria Paunescu100% (2)
- Spinal Cord Injury: Causation & PathophysiologyDocument10 pagesSpinal Cord Injury: Causation & Pathophysiologycpradheep100% (3)
- Of The Abdominal Wall, Abdominal Organs, Vasculature, Spinal Nerves and DermatomesDocument11 pagesOf The Abdominal Wall, Abdominal Organs, Vasculature, Spinal Nerves and DermatomesentistdeNo ratings yet
- Bogduk Meniscoide PDFDocument15 pagesBogduk Meniscoide PDFMatias Hassan LattzNo ratings yet
- Block 4 OPP Lecture NotesDocument59 pagesBlock 4 OPP Lecture Notesjeremy_raineyNo ratings yet
- Ajr.09.2772 Grading Neuroforaminal StenosisDocument4 pagesAjr.09.2772 Grading Neuroforaminal StenosisOscar NogueraNo ratings yet
- Vol I - Oase, Articulatii, Ligamente Si Muschi PDFDocument454 pagesVol I - Oase, Articulatii, Ligamente Si Muschi PDFBianca Byby100% (1)
- Spinal Injuries ProgramDocument9 pagesSpinal Injuries ProgramIslam AminNo ratings yet
- Widya - Basic Lumbal Spine MriDocument31 pagesWidya - Basic Lumbal Spine MriPrabaningrum DwidjoasmoroNo ratings yet
- Kidney Dystopia Cherupuratt Adershraj 426bDocument21 pagesKidney Dystopia Cherupuratt Adershraj 426bAdarsha SubramanianNo ratings yet
- Vertebra Anatomy 125Document110 pagesVertebra Anatomy 125Jennifer FirestoneNo ratings yet
- Mechanical Properties of Lumbar Spine Motion Segments Under Large LoadsDocument6 pagesMechanical Properties of Lumbar Spine Motion Segments Under Large LoadsMike Vandumurugan100% (1)
- Patterns of Spinal Motion During Walking: Jack Crosbie ", Roongtiwa Vachalathitib, Richard Smith"Document7 pagesPatterns of Spinal Motion During Walking: Jack Crosbie ", Roongtiwa Vachalathitib, Richard Smith"Patrik NazarioNo ratings yet
- Lower Back Pain and DisordersDocument74 pagesLower Back Pain and DisordersZdenek93No ratings yet
- Total Postural Reprogramming: 3rd EditionDocument21 pagesTotal Postural Reprogramming: 3rd EditionXXXXXXXX50% (2)
- Ana-Physio (Reviewer For Grade 12 Students in Asia)Document20 pagesAna-Physio (Reviewer For Grade 12 Students in Asia)James Yap LimboyNo ratings yet
- SpondylolisthesisDocument22 pagesSpondylolisthesisgonsteadtruth100% (3)
- Back Spine AnatomyDocument3 pagesBack Spine AnatomyNinjaNo ratings yet
- Omm Technique ListDocument2 pagesOmm Technique ListEman ElzeftawyNo ratings yet