You might also like
- Stroke PathophysiologyDocument3 pagesStroke PathophysiologyMaureen EricaNo ratings yet
- Pathophysiology CVD InfarctDocument1 pagePathophysiology CVD InfarctElisa KerrNo ratings yet
- Pathophysiology of StrokeDocument4 pagesPathophysiology of StrokeACe JAyNo ratings yet
- Sepsis Is The Consequence of A Dysregulated Inflammatory Response To An Infectious InsultDocument11 pagesSepsis Is The Consequence of A Dysregulated Inflammatory Response To An Infectious InsultShrests SinhaNo ratings yet
- Pathophysiology of CVADocument1 pagePathophysiology of CVAChristine Joy Ilao PasnoNo ratings yet
- Pathophysiology CVADocument1 pagePathophysiology CVANenette Aquino100% (2)
- Pathophysiology ErDocument3 pagesPathophysiology ErAlexa A. AldayNo ratings yet
- Pathophysiology in Liver CirrhosisDocument4 pagesPathophysiology in Liver CirrhosisCyrus Ortalla RobinNo ratings yet
- Pa Tho Physiology of Hemorrhagic StrokeDocument2 pagesPa Tho Physiology of Hemorrhagic StrokeMerlash MerlaNo ratings yet
- Heart Failure COncept MapDocument2 pagesHeart Failure COncept MapJrBong SemaneroNo ratings yet
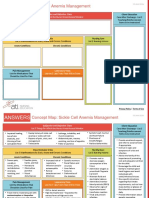
- NCC-SickleCellAnemiaManagement ConceptMap InteractivePDFDocument2 pagesNCC-SickleCellAnemiaManagement ConceptMap InteractivePDFLoggerz Arck100% (1)
- Pathophysiology and Schematic Diagram of Typhoid FeverDocument3 pagesPathophysiology and Schematic Diagram of Typhoid FeverCyrus De AsisNo ratings yet
- PathophysiologyDocument34 pagesPathophysiologyeunams_1195% (20)
- Pathophysiology CHFDocument2 pagesPathophysiology CHFPerry Oliver AlvarezNo ratings yet
- Pathophysiology HPN CvaDocument1 pagePathophysiology HPN Cvatresdos09No ratings yet
- Pathophysiology: Precipitating FactorDocument6 pagesPathophysiology: Precipitating FactorMark Anthony YabresNo ratings yet
- "Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyDocument3 pages"Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Client Centered PathophysiologyCarl Elexer Cuyugan Ano50% (2)
- CellulitisDocument39 pagesCellulitisMary Jhane Villanueva50% (4)
- Stroke PathophysiologyDocument2 pagesStroke PathophysiologyJaessa Feliciano100% (2)
- Cholecystitis Nursing Care PlanDocument4 pagesCholecystitis Nursing Care PlanMDCITY83% (6)
- Schematic Pathophysiology CVADocument10 pagesSchematic Pathophysiology CVAheiyu100% (5)
- Guillain Barre Syndrome PathophysiologyDocument4 pagesGuillain Barre Syndrome Pathophysiologykathy100% (13)
- Drug Study Case 1Document37 pagesDrug Study Case 1Maria Charis Anne IndananNo ratings yet
- Age Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat IntakeDocument3 pagesAge Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat Intakenursing concept mapsNo ratings yet
- Angina Pectoris PathophysiologyDocument2 pagesAngina Pectoris PathophysiologyALIANA KIMBERLY MALQUESTONo ratings yet
- Qtsoi Concept MapDocument5 pagesQtsoi Concept MapGenella BabantoNo ratings yet
- Pathophysiology of TiaDocument1 pagePathophysiology of Tiaabbeeyy100% (1)
- Concept MapDocument1 pageConcept MapChristine Marie Barce Martinez100% (2)
- Case On Intracranial HemorrhageDocument17 pagesCase On Intracranial HemorrhageLorebell100% (2)
- Pathophysiology of Congestive Heart FailureDocument3 pagesPathophysiology of Congestive Heart Failuretinayko100% (1)
- Final patho-HCVDDocument2 pagesFinal patho-HCVDAlvin RamirezNo ratings yet
- Concept MapDocument5 pagesConcept Mapmild_tea100% (1)
- Transient Ischemic AttackDocument7 pagesTransient Ischemic AttackJennifer DimapilisNo ratings yet
- Pathophysiology of Meniere FinalDocument1 pagePathophysiology of Meniere Final1S VILLEGAS GabrielNo ratings yet
- DB13 - Pathophysiology of AtherosclerosisDocument2 pagesDB13 - Pathophysiology of Atherosclerosisi_vhie03No ratings yet
- Ineffective Tissue Perfusion PDFDocument4 pagesIneffective Tissue Perfusion PDFgcodouganNo ratings yet
- Pathophysiology of Leptospirosis and Dengue FeverDocument5 pagesPathophysiology of Leptospirosis and Dengue FeverKenneth Lagman100% (1)
- CVA PathophysiologyDocument3 pagesCVA Pathophysiologyshmily_0810No ratings yet
- Pathophysiology Sickle Cell Anemia PDFDocument1 pagePathophysiology Sickle Cell Anemia PDFTine GuibaoNo ratings yet
- Acute Coronary SyndromeDocument2 pagesAcute Coronary SyndromeRenz Castañaday100% (1)
- Pathophysiology of DMDocument4 pagesPathophysiology of DMNicole Louise N. VillanuevaNo ratings yet
- Pathophysiology of Diabetes Mellitus Type 2Document1 pagePathophysiology of Diabetes Mellitus Type 2faula rocamora100% (3)
- Pathophysiology of Status EpilepticusDocument6 pagesPathophysiology of Status EpilepticusKysha Ruth SevillaNo ratings yet
- Cva NCPDocument2 pagesCva NCPSharewin PulidoNo ratings yet
- Pathophysiology Hemorrhagic StrokeDocument1 pagePathophysiology Hemorrhagic StrokeJeffrey Dela CruzNo ratings yet
- Stroke PathophysiologyDocument5 pagesStroke Pathophysiologycinnabon_heart9100% (3)
- Pathophysiology of AppendicitisDocument2 pagesPathophysiology of Appendicitis33342No ratings yet
- COPD PathophysiologyDocument1 pageCOPD Pathophysiologyaj ajNo ratings yet
- COPD PathophysiologyDocument1 pageCOPD PathophysiologyJustin Ahorro-Dionisio33% (3)
- Systemic Lupus Erythematosus (SLE) : Genetic Factors Environmental FactorsDocument5 pagesSystemic Lupus Erythematosus (SLE) : Genetic Factors Environmental Factorsjoyrena ochondraNo ratings yet
- Precipitating Factors Predisposing Factors Chronic Kidney DiseaseDocument3 pagesPrecipitating Factors Predisposing Factors Chronic Kidney DiseaseGrace Jane DionaldoNo ratings yet
- STROKE: Handbook with activities, exercises and mental challengesFrom EverandSTROKE: Handbook with activities, exercises and mental challengesNo ratings yet
- What Is A StrokeDocument5 pagesWhat Is A StrokeLintsuNo ratings yet
- Focus On StrokeDocument92 pagesFocus On StrokeDIAH RETNO WULAN100% (2)
- Case 1 FinalDocument70 pagesCase 1 FinalMaria Charis Anne IndananNo ratings yet
- Cerebrovascular Diseas1Document47 pagesCerebrovascular Diseas1Jenard Joniel OlivarNo ratings yet
- Cerebrovascular Accident: Silliman University Dumaguete City Resource Unit OnDocument18 pagesCerebrovascular Accident: Silliman University Dumaguete City Resource Unit OnCharles KevinNo ratings yet
- Cross StitchDocument1 pageCross StitchMark Anthony Taña GabiosaNo ratings yet
- Drug StudyDocument7 pagesDrug StudyMark Anthony Taña GabiosaNo ratings yet
- Differents Kind of Mountain and HillDocument8 pagesDifferents Kind of Mountain and HillMark Anthony Taña GabiosaNo ratings yet
- Longitude Is A Geographic Coordinate That Specifies The EastDocument1 pageLongitude Is A Geographic Coordinate That Specifies The EastMark Anthony Taña GabiosaNo ratings yet
- Agn PediaDocument5 pagesAgn PediaMark Anthony Taña GabiosaNo ratings yet
- If Things DonDocument1 pageIf Things DonMark Anthony Taña GabiosaNo ratings yet
- If Things DonDocument1 pageIf Things DonMark Anthony Taña GabiosaNo ratings yet
- MefenamicDocument2 pagesMefenamicMark Anthony Taña GabiosaNo ratings yet
- 5 Biomechanics of Elbow JointDocument45 pages5 Biomechanics of Elbow JointJHINUK DASGUPTANo ratings yet
- Deep Tendon Reflex Steps On How To Assess The DTR: Normal Response: DTR GradingDocument2 pagesDeep Tendon Reflex Steps On How To Assess The DTR: Normal Response: DTR GradingElla EvangelistaNo ratings yet
- Properties of Cardiac Muscle PDFDocument38 pagesProperties of Cardiac Muscle PDFZaid RazaliNo ratings yet
- HOPE 2A MODULE 4 Badminton 2 PDFDocument19 pagesHOPE 2A MODULE 4 Badminton 2 PDFLeo Patrick100% (7)
- Circulatory SystemDocument3 pagesCirculatory Systemnacuamaryjoy123No ratings yet
- Lab Muscle ContractionDocument5 pagesLab Muscle ContractionAllan DuplaNo ratings yet
- Post Mastectomy ExerciseDocument4 pagesPost Mastectomy ExerciseKusum RoyNo ratings yet
- SkullDocument23 pagesSkullurjaNo ratings yet
- Interdigital (Morton's) Neuroma - Foot & Ankle - OrthobulletsDocument3 pagesInterdigital (Morton's) Neuroma - Foot & Ankle - OrthobulletsEmiel AwadNo ratings yet
- Tubular and Massif Organ: Problem Based Learning (PBL)Document18 pagesTubular and Massif Organ: Problem Based Learning (PBL)KEZIA CALISTA HERLIANINo ratings yet
- Ch. 4 TissuesDocument55 pagesCh. 4 TissuesBora YaNo ratings yet
- Keilhauer Sguig BrochureDocument11 pagesKeilhauer Sguig BrochureJeffrey MeltzerNo ratings yet
- Oral Anatomy Q&ADocument8 pagesOral Anatomy Q&AHanny CarinoNo ratings yet
- Untamed MDMW Home 1-2Document5 pagesUntamed MDMW Home 1-2Leena FranklinNo ratings yet
- Hormones: Test Yourself 15.1 (Page 287)Document3 pagesHormones: Test Yourself 15.1 (Page 287)leeNo ratings yet
- Riumachi 31Document7 pagesRiumachi 31tommy58No ratings yet
- Skin Flap Physiology PDFDocument25 pagesSkin Flap Physiology PDFTang Weng JunNo ratings yet
- Baza III Curs MedDocument117 pagesBaza III Curs MedIntekhabAtahar0% (1)
- Factores Macroesteticos en El Diseño de SonrisaDocument7 pagesFactores Macroesteticos en El Diseño de SonrisaJassel DurdenNo ratings yet
- Physiological Modeling - Final Project (Circulatory System)Document18 pagesPhysiological Modeling - Final Project (Circulatory System)Joshua DamianNo ratings yet
- Exclusive 42 BCS Solve SheetDocument272 pagesExclusive 42 BCS Solve SheetRezaul RazibNo ratings yet
- Case Study On Tos & Cervical Stenosis: by Faviola Bedoy, SPTADocument14 pagesCase Study On Tos & Cervical Stenosis: by Faviola Bedoy, SPTAapi-547954700No ratings yet
- Biomechanics of Knee JointDocument123 pagesBiomechanics of Knee JointSIBASIS PATTANAYAKNo ratings yet
- Ha&P - Semi ReviewerDocument71 pagesHa&P - Semi ReviewerLittle StuartNo ratings yet
- Gym PrinciplesDocument23 pagesGym PrinciplesKrešimir DodigNo ratings yet
- Spinal NervesDocument53 pagesSpinal Nervespearl joy holleroNo ratings yet
- Maxillary SinusDocument37 pagesMaxillary SinusSkAliHassan100% (2)
- Sensory Systems Lecture NotesDocument7 pagesSensory Systems Lecture Notesdevilstrill1605100% (1)
- Amphibian Anatomy and PhysiologyDocument10 pagesAmphibian Anatomy and PhysiologySilvi SiNo ratings yet
- Nursing Head-to-Toe Assessment Cheat Sheet PDFDocument7 pagesNursing Head-to-Toe Assessment Cheat Sheet PDFJoebert BangsoyNo ratings yet