You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 952-Article Text-3024-1-10-20221113Document13 pages952-Article Text-3024-1-10-20221113Audi GaluhNo ratings yet
- The Salesman Analysis by Tanmay TandonDocument2 pagesThe Salesman Analysis by Tanmay TandonTanmay TandonNo ratings yet
- HTM - 05-03 - Part - C (Textiles & Furnishing)Document66 pagesHTM - 05-03 - Part - C (Textiles & Furnishing)afadlallaNo ratings yet
- Improve Patient Safety by Reducing Medication ErrorsDocument95 pagesImprove Patient Safety by Reducing Medication Errorsdev5683No ratings yet
- Security Assessment &recommendation: PurposeDocument3 pagesSecurity Assessment &recommendation: PurposeEricka W.No ratings yet
- BSBPMG536 - Manage Project Risk: Week 5Document9 pagesBSBPMG536 - Manage Project Risk: Week 5usama sarwerNo ratings yet
- Transcultural Nursing Theories - Leininger and OremDocument22 pagesTranscultural Nursing Theories - Leininger and OremArah Lyn ApiagNo ratings yet
- Soac 2021 First AnnouncementDocument13 pagesSoac 2021 First AnnouncementHendi PrihatnaNo ratings yet
- Surgical Intern Manual (For Pre-Intern) QEHDocument10 pagesSurgical Intern Manual (For Pre-Intern) QEHChris Jardine LiNo ratings yet
- Pilot II: Technical Data SheetDocument4 pagesPilot II: Technical Data SheetSafinahNo ratings yet
- 2 Prenatal CareDocument19 pages2 Prenatal CareShahina ShayneNo ratings yet
- How to Cite Patient Safety Incident Reporting SystemDocument7 pagesHow to Cite Patient Safety Incident Reporting System'Amel'AyuRizkyAmeliyahNo ratings yet
- Education and HealthDocument4 pagesEducation and Healthsagar111033No ratings yet
- KHDA - Dar Al Marefa School 2016-2017Document27 pagesKHDA - Dar Al Marefa School 2016-2017Edarabia.comNo ratings yet
- BBMP Birth & Death Certificate FAQsDocument4 pagesBBMP Birth & Death Certificate FAQsindian250% (1)
- Behavioural Changes After Anaesthesia: Validity and Liability of The Post Hospitalization Behavior Questionnaire in A Swedish Paediatric PopulationDocument8 pagesBehavioural Changes After Anaesthesia: Validity and Liability of The Post Hospitalization Behavior Questionnaire in A Swedish Paediatric PopulationLakhwinder KaurNo ratings yet
- Male, Masculinities Methodologies and MethodsDocument40 pagesMale, Masculinities Methodologies and MethodsMarco Rojas VNo ratings yet
- Mam TAtaDocument7 pagesMam TAtaRAZEL C. SORIANO, MSciEdNo ratings yet
- COPSOQ III Questionnaire 060718Document6 pagesCOPSOQ III Questionnaire 060718Beatriz Barboza VeraNo ratings yet
- Mothers Should Have Custody of Illegitimate ChildDocument1 pageMothers Should Have Custody of Illegitimate Childalwayskeepthefaith8No ratings yet
- Asthma Guidelines in Philippines PDFDocument91 pagesAsthma Guidelines in Philippines PDFxtine100% (2)
- IHKS Summit ProgramDocument35 pagesIHKS Summit ProgramDiah Rahayu SetiawatiNo ratings yet
- Action Planning For ToRs of CMT - XLSX CompleteDocument1 pageAction Planning For ToRs of CMT - XLSX CompleteOSCAR RUHWEZANo ratings yet
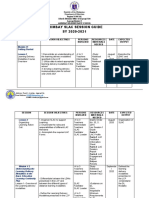
- Arimbay Slac Session Guide SY 2020-2021Document6 pagesArimbay Slac Session Guide SY 2020-2021Jen ApinadoNo ratings yet
- Chapter One 1.1 Background To The StudyDocument6 pagesChapter One 1.1 Background To The Studyhis excellencyNo ratings yet
- Topnotch Surgery Reviewer PDFDocument81 pagesTopnotch Surgery Reviewer PDFkat0% (1)
- Central Mindanao University College of Nursing NGT Insertion ProcedureDocument3 pagesCentral Mindanao University College of Nursing NGT Insertion ProcedureDARWIN JAY SANG-ANNo ratings yet
- 2020 GPB - Revised FormDocument32 pages2020 GPB - Revised FormJoseph Caballero CruzNo ratings yet
- Annotated BibliographyDocument2 pagesAnnotated Bibliographyapi-708978172No ratings yet
- Higher Nationals in Computing: Unit 06: Managing A Successful Computing Project Assignment 1Document27 pagesHigher Nationals in Computing: Unit 06: Managing A Successful Computing Project Assignment 1nhan leNo ratings yet