You might also like
- Jcpe 12078Document12 pagesJcpe 12078SitiKhadijahNo ratings yet
- Biological Width May 2013Document12 pagesBiological Width May 2013Bogdan MunteanuNo ratings yet
- Indices To Assess Malocclusions in Patients With Cleft Lip and Palate PDFDocument11 pagesIndices To Assess Malocclusions in Patients With Cleft Lip and Palate PDFIsharajini Prasadika Subhashni GamageNo ratings yet
- Soft Tissue Changes Following Extraction vs. Nonextraction Orthodontic Fixed Appliance Treatment: A Systematic Review and Meta-AnalysisDocument13 pagesSoft Tissue Changes Following Extraction vs. Nonextraction Orthodontic Fixed Appliance Treatment: A Systematic Review and Meta-AnalysisqwertygalNo ratings yet
- I1945-7103-92-2-275 Clear AlignerDocument12 pagesI1945-7103-92-2-275 Clear AlignerLima JúniorNo ratings yet
- Papadopoulos 2007Document18 pagesPapadopoulos 2007ReshamIrshadNo ratings yet
- TL3 8 Garbim2021Document33 pagesTL3 8 Garbim2021bomonnhacongdongNo ratings yet
- Evidence-Based Dentistry. How To Design A Research? A Literature ReviewDocument7 pagesEvidence-Based Dentistry. How To Design A Research? A Literature ReviewNadya ANo ratings yet
- Weijden Et Al-2015-Journal of Clinical Periodontology PDFDocument15 pagesWeijden Et Al-2015-Journal of Clinical Periodontology PDFChristine HacheNo ratings yet
- Effectiveness of Biologic Methods of Inhibiting Orthodontic Tooth Movement in Animal StudiesDocument16 pagesEffectiveness of Biologic Methods of Inhibiting Orthodontic Tooth Movement in Animal StudiesHusni mubarakNo ratings yet
- Periodontal Health During Orthodontic Treatment With Clear Aligners and Fixed AppliancesDocument21 pagesPeriodontal Health During Orthodontic Treatment With Clear Aligners and Fixed AppliancesabocoliNo ratings yet
- Guy Huynh-Ba 2018Document15 pagesGuy Huynh-Ba 2018IsmaelNo ratings yet
- Dentistry 11 00046 v2Document18 pagesDentistry 11 00046 v2MARTÍN EMILIO BENAVENTENo ratings yet
- Baccaglini Et Al 2010Document9 pagesBaccaglini Et Al 2010Amanda AiresNo ratings yet
- DinaDocument8 pagesDinadinaNo ratings yet
- Martini 2021Document17 pagesMartini 2021Matheus JacobinaNo ratings yet
- Orthodontic Anchorage A Systematic ReviewDocument9 pagesOrthodontic Anchorage A Systematic ReviewIvanna H. A.No ratings yet
- Association Between Malocclusion and Dental Caries in Adolescents: A Systematic Review and Meta AnalysisDocument10 pagesAssociation Between Malocclusion and Dental Caries in Adolescents: A Systematic Review and Meta AnalysisRoxana OneaNo ratings yet
- Quality Assessment of Systematic Reviews On Alveolar Socket Preservation.Document9 pagesQuality Assessment of Systematic Reviews On Alveolar Socket Preservation.andreita_loppNo ratings yet
- Third Molar Surgical Difficulty Scales: Systematic Review and Preoperative Assessment FormDocument9 pagesThird Molar Surgical Difficulty Scales: Systematic Review and Preoperative Assessment FormdaruNo ratings yet
- The Role of Triage Nurse Ordering. Brian H. Rowe, 2011 PDFDocument9 pagesThe Role of Triage Nurse Ordering. Brian H. Rowe, 2011 PDFCristobal Alejandro Falado SantanderNo ratings yet
- Potential Errors and Misuse of Statistics in StudiesDocument9 pagesPotential Errors and Misuse of Statistics in StudiesAbad SalcedoNo ratings yet
- Early Orthodontic Treatment of Skeletal Open-Bite MalocclusionDocument7 pagesEarly Orthodontic Treatment of Skeletal Open-Bite MalocclusionMaria SilvaNo ratings yet
- Nueva Propuestata Diagnóstico EndodonticoDocument10 pagesNueva Propuestata Diagnóstico EndodonticoNatali ZBravoNo ratings yet
- Antibiotic Prophylaxis in Orthognathic Surgery - An Overview of Systematic ReviewsDocument12 pagesAntibiotic Prophylaxis in Orthognathic Surgery - An Overview of Systematic ReviewsBruno GuardieiroNo ratings yet
- NG 2007Document19 pagesNG 2007NunoGonçalvesNo ratings yet
- Examiner Alignment and Assessment in Clinical Periodontal Researchhefti - Et - Al-2012-Periodontology - 2000Document20 pagesExaminer Alignment and Assessment in Clinical Periodontal Researchhefti - Et - Al-2012-Periodontology - 2000Dr. DeeptiNo ratings yet
- Validity Two Methods For Assessing Oral Health Status of PopulationsDocument9 pagesValidity Two Methods For Assessing Oral Health Status of PopulationsSyarifah HaizanNo ratings yet
- FIGO Clasificación HUA 2011Document11 pagesFIGO Clasificación HUA 2011dickenskevinNo ratings yet
- The Impact of Sealer Extrusion On Endodontic Outcome: A Systematic Review With Meta-AnalysisDocument7 pagesThe Impact of Sealer Extrusion On Endodontic Outcome: A Systematic Review With Meta-Analysisitsme543210No ratings yet
- Cognitive Behaviour Therapy For Anxious Paediatric Dental Patients: A Systematic ReviewDocument10 pagesCognitive Behaviour Therapy For Anxious Paediatric Dental Patients: A Systematic ReviewSung Soon ChangNo ratings yet
- Management of Post-Orthodontic White Spot Lesions: An Updated Systematic ReviewDocument6 pagesManagement of Post-Orthodontic White Spot Lesions: An Updated Systematic ReviewRiska Endah CahyaniNo ratings yet
- FIGOCEDocument11 pagesFIGOCEAldwin TanuwijayaNo ratings yet
- Qi 51 2 Rososorio p100Document8 pagesQi 51 2 Rososorio p100AKSNo ratings yet
- Efectos AdversosDocument10 pagesEfectos Adversosjeimmy dulceyNo ratings yet
- Performing A Literature Review BMJDocument8 pagesPerforming A Literature Review BMJfvgrsm8r100% (1)
- Angle 2007 Vol. 77, No. 2, Pp. 376-381Document6 pagesAngle 2007 Vol. 77, No. 2, Pp. 376-381André MéndezNo ratings yet
- 10.1007@s00784 020 03415 0Document14 pages10.1007@s00784 020 03415 0Alison ContrerasNo ratings yet
- ARTÍCULO BASE Valkenburg2019Document12 pagesARTÍCULO BASE Valkenburg2019Andrea LopezNo ratings yet
- Risk Factors For Early Childhood Caries: A Systematic Review and Meta-Analysis of Case Control and Cohort StudiesDocument18 pagesRisk Factors For Early Childhood Caries: A Systematic Review and Meta-Analysis of Case Control and Cohort StudiesNatalia DavilaNo ratings yet
- Apraxia TXDocument20 pagesApraxia TXadriricaldeNo ratings yet
- Global Distribution of Malocclusion Traits: A Systematic ReviewDocument10 pagesGlobal Distribution of Malocclusion Traits: A Systematic ReviewRoxana OneaNo ratings yet
- Gagnier2012 - Investigating CHDocument15 pagesGagnier2012 - Investigating CHrestu pangestutiNo ratings yet
- 2022 Aburas - Dentophobia and Dental Treatment An Umbrella Review of The PublishedDocument11 pages2022 Aburas - Dentophobia and Dental Treatment An Umbrella Review of The Publishedfabian.balazs.93No ratings yet
- Clinical Effectiveness of Invisalign® Orthodontic Treatment: A Systematic ReviewDocument24 pagesClinical Effectiveness of Invisalign® Orthodontic Treatment: A Systematic ReviewMario AdánNo ratings yet
- 10 1016@j Jebdp 2020 101402Document18 pages10 1016@j Jebdp 2020 101402ali asiriNo ratings yet
- Sclerotherapy For Hemorrhoidal Disease: Systematic Review and Meta AnalysisDocument11 pagesSclerotherapy For Hemorrhoidal Disease: Systematic Review and Meta Analysistheomnagarowner2811No ratings yet
- 2019 WedadDocument8 pages2019 Wedadnermal93No ratings yet
- Knowledge of European Orthodontic Postgraduate Students On BiostatisticsDocument7 pagesKnowledge of European Orthodontic Postgraduate Students On BiostatisticshemaadriNo ratings yet
- Factors Affecting Irrigant Extrusion During Root Canal Irrigation A Systematic ReviewDocument20 pagesFactors Affecting Irrigant Extrusion During Root Canal Irrigation A Systematic ReviewFernando CordovaNo ratings yet
- Amino Sharia e 2017Document6 pagesAmino Sharia e 2017Heba AtefNo ratings yet
- Measuring Oral Health and Quality of LifeDocument172 pagesMeasuring Oral Health and Quality of LifeCalin Dragoman100% (1)
- Soft-Tissue Changes in Class II Malocclusion Patients Treated With Extractions: A Systematic ReviewDocument7 pagesSoft-Tissue Changes in Class II Malocclusion Patients Treated With Extractions: A Systematic ReviewAndrea GamezNo ratings yet
- Caries DiagnosisDocument6 pagesCaries DiagnosisAbhishek SoniNo ratings yet
- Angle Orthod. 2015 85 5 881-9Document9 pagesAngle Orthod. 2015 85 5 881-9brookortontiaNo ratings yet
- Martinez 2020 COLORDocument20 pagesMartinez 2020 COLORAnonymous AyxIccS4aXNo ratings yet
- Analysis of Clinical Trials Using SAS: A Practical Guide, Second EditionFrom EverandAnalysis of Clinical Trials Using SAS: A Practical Guide, Second EditionNo ratings yet
- Practical Oncologic Molecular Pathology: Frequently Asked QuestionsFrom EverandPractical Oncologic Molecular Pathology: Frequently Asked QuestionsNo ratings yet
- Practical Biostatistics: A Friendly Step-by-Step Approach for Evidence-based MedicineFrom EverandPractical Biostatistics: A Friendly Step-by-Step Approach for Evidence-based MedicineRating: 5 out of 5 stars5/5 (1)
- Temperature Rise of The Post & On The Root Surface During Ultrasonic Post RemovalDocument7 pagesTemperature Rise of The Post & On The Root Surface During Ultrasonic Post RemovalNoor Al-Deen MaherNo ratings yet
- JurnalDocument5 pagesJurnalSeptina Anggun PNo ratings yet
- Root End Filling Materials - A ReviewDocument19 pagesRoot End Filling Materials - A ReviewFlorin IonescuNo ratings yet
- Root Canal Instruments For Manual Use - A ReviewDocument15 pagesRoot Canal Instruments For Manual Use - A ReviewFlorin IonescuNo ratings yet
- Prognosis of Luxated Permanent Teeth - The Development of Pulp NecrosisDocument15 pagesPrognosis of Luxated Permanent Teeth - The Development of Pulp NecrosisFlorin IonescuNo ratings yet
- Reasons For Apicectomies A Retrospective StudyDocument8 pagesReasons For Apicectomies A Retrospective StudyFlorin IonescuNo ratings yet
- Radio Graphic Evaluation of Cases Referred For Surgical TicsDocument6 pagesRadio Graphic Evaluation of Cases Referred For Surgical TicsFlorin IonescuNo ratings yet
- Similarities in The Micro Floras of Root Canals and Deep Periodontal PocketsDocument6 pagesSimilarities in The Micro Floras of Root Canals and Deep Periodontal PocketsFlorin IonescuNo ratings yet
- Root Canal Treatment and General Health - A Review of The LiteratureDocument18 pagesRoot Canal Treatment and General Health - A Review of The LiteratureFlorin IonescuNo ratings yet
- Review of The Current Status of Tooth Whitening With The Walking Bleach TechniqueDocument17 pagesReview of The Current Status of Tooth Whitening With The Walking Bleach TechniqueFlorin IonescuNo ratings yet
- Prognosis of Permanent Teeth With Internal Resorption - A Clinical ReviewDocument8 pagesPrognosis of Permanent Teeth With Internal Resorption - A Clinical ReviewFlorin IonescuNo ratings yet
- Prevalence of Persistent Pain After Tic Treatment and Factors Affecting Its Occurrence inDocument10 pagesPrevalence of Persistent Pain After Tic Treatment and Factors Affecting Its Occurrence inFlorin IonescuNo ratings yet
- Retrograde Approaches in Tic TherapyDocument12 pagesRetrograde Approaches in Tic TherapyFlorin IonescuNo ratings yet
- Pulp Capping With Adhesive Resin-Based Composite vs. Calcium Hydroxide - A ReviewDocument11 pagesPulp Capping With Adhesive Resin-Based Composite vs. Calcium Hydroxide - A ReviewFlorin IonescuNo ratings yet
- Radio Graphic Study of The Effect of Various Retrograde Fillings On Periapical Healing After ReplaDocument7 pagesRadio Graphic Study of The Effect of Various Retrograde Fillings On Periapical Healing After ReplaFlorin IonescuNo ratings yet
- Periodontal Ligament Anesthesia - A Clinical EvaluationDocument4 pagesPeriodontal Ligament Anesthesia - A Clinical EvaluationFlorin IonescuNo ratings yet
- Periapical Radiolucency Mimicking An Odontogenic CystDocument8 pagesPeriapical Radiolucency Mimicking An Odontogenic CystFlorin IonescuNo ratings yet
- Post-Traumatic Use of Dental Implants To Rehabilitate Anterior Maxillary TeethDocument4 pagesPost-Traumatic Use of Dental Implants To Rehabilitate Anterior Maxillary TeethFlorin Ionescu100% (1)
- Periodontal Destruction and Tooth Loss Following Pulp Devitalization With ToxavitDocument7 pagesPeriodontal Destruction and Tooth Loss Following Pulp Devitalization With ToxavitFlorin IonescuNo ratings yet
- Paget's Disease of The Mandible - A Review and Report of A CaseDocument5 pagesPaget's Disease of The Mandible - A Review and Report of A CaseFlorin IonescuNo ratings yet
- Periapical Actinomycosis Report of A Case and Review of The LiteratureDocument5 pagesPeriapical Actinomycosis Report of A Case and Review of The LiteratureFlorin IonescuNo ratings yet
- Periapical Radiolucencies As Evaluated by Bisecting-Angle and Paralleling Radio Graphic TechniquesDocument9 pagesPeriapical Radiolucencies As Evaluated by Bisecting-Angle and Paralleling Radio Graphic TechniquesFlorin Ionescu100% (1)
- Or Tho Grade Re Treatment and Apexification After Unsuccessful Tic Treatment, Re Treatment andDocument7 pagesOr Tho Grade Re Treatment and Apexification After Unsuccessful Tic Treatment, Re Treatment andFlorin IonescuNo ratings yet
- Periapical Central Giant Cell Granuloma Misdiagnosed As Odontogenic CystDocument6 pagesPeriapical Central Giant Cell Granuloma Misdiagnosed As Odontogenic CystFlorin IonescuNo ratings yet
- Microbiota of Periapical Lesions Refractory ToDocument7 pagesMicrobiota of Periapical Lesions Refractory ToFlorin IonescuNo ratings yet
- Micro Surgical Instruments For Root-End Cavity Preparation Following Apicoectomy A Literature RevDocument16 pagesMicro Surgical Instruments For Root-End Cavity Preparation Following Apicoectomy A Literature RevFlorin IonescuNo ratings yet
- On The Causes of Persistent Apical Period On Tit Is - A ReviewDocument33 pagesOn The Causes of Persistent Apical Period On Tit Is - A ReviewFlorin IonescuNo ratings yet
- Multiple Dental Fractures Following Tongue Barbell Placement - A Case ReportDocument3 pagesMultiple Dental Fractures Following Tongue Barbell Placement - A Case ReportFlorin IonescuNo ratings yet
- Flare Ups SiqueiraDocument11 pagesFlare Ups SiqueiraHadil AltilbaniNo ratings yet
- Microbial Micro Leakage and Pulpal Inflammation - A ReviewDocument8 pagesMicrobial Micro Leakage and Pulpal Inflammation - A ReviewFlorin IonescuNo ratings yet
- RPH PDPR 2-4 OgosDocument2 pagesRPH PDPR 2-4 OgosLAILI ATIQAH BINTI JIHAT MoeNo ratings yet
- National Institute of Rural Development & Panchayati RajDocument13 pagesNational Institute of Rural Development & Panchayati Rajsevalal vkbNo ratings yet
- Toby Carroll - Neoliberal Development Policy in AsiaDocument85 pagesToby Carroll - Neoliberal Development Policy in AsiaINFID JAKARTANo ratings yet
- 09 Registered Teacher Criteria SelfDocument15 pages09 Registered Teacher Criteria Selfapi-300095367No ratings yet
- I. Facts of The Case: Confetti ShoesDocument5 pagesI. Facts of The Case: Confetti ShoesJessuel Larn-epsNo ratings yet
- Estudio Social e Intercultural Del Lenguaje, La Personalidad y La Medición Del Sistema (Motivacional) A-R-D HumanoDocument90 pagesEstudio Social e Intercultural Del Lenguaje, La Personalidad y La Medición Del Sistema (Motivacional) A-R-D HumanoWilliam Montgomery UrdayNo ratings yet
- DTL Assignment2Document18 pagesDTL Assignment2api-466686358No ratings yet
- Prepare A Report On Study of Management Applied To Small Scale IndustryDocument7 pagesPrepare A Report On Study of Management Applied To Small Scale Industry05 Pratiksha BangarNo ratings yet
- Marking scheme and topics for CBSE Class 12 English Core board examDocument17 pagesMarking scheme and topics for CBSE Class 12 English Core board examRonaldNo ratings yet
- A Study On Working Women and Their InvestmentDocument70 pagesA Study On Working Women and Their InvestmentRITIKA PATHAKNo ratings yet
- ISTQB ATA (Advanced Test Analyst) Certification Exam Practice Questions For Testing ProcessDocument10 pagesISTQB ATA (Advanced Test Analyst) Certification Exam Practice Questions For Testing ProcessShanthi Kumar Vemulapalli100% (1)
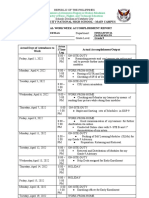
- Cotabato City National High School - Main Campus Individual Workweek Accomplishment ReportDocument3 pagesCotabato City National High School - Main Campus Individual Workweek Accomplishment ReportAmi RANo ratings yet
- No IELTS Canada GuideDocument4 pagesNo IELTS Canada GuideOluwadamilola Shitta-beyNo ratings yet
- Primary, Secondary and Tertiary Sources in The Health SciencesDocument3 pagesPrimary, Secondary and Tertiary Sources in The Health SciencesBMohdIshaqNo ratings yet
- House Bill 1557 (Don't Say Gay)Document4 pagesHouse Bill 1557 (Don't Say Gay)Michelle Solomon50% (2)
- Lungu - How About Intercomprehension - Different IC ProjectsDocument4 pagesLungu - How About Intercomprehension - Different IC ProjectsAnna NekrasovaNo ratings yet
- Classhome Program for Grade 1Document1 pageClasshome Program for Grade 1Jazmen Madrigal LlarenaNo ratings yet
- Poblacion 3, Gerona, Tarlac Senior High School DepartmentDocument6 pagesPoblacion 3, Gerona, Tarlac Senior High School DepartmentMarvin Dagdag MoralesNo ratings yet
- A. Reviewing Previous Lesson or Presenting The New LessonDocument3 pagesA. Reviewing Previous Lesson or Presenting The New LessonJanice Carnate CataggatanNo ratings yet
- I. Objectives: Mga Isyung Pangkapaligiran at Pang-EkonomiyaDocument4 pagesI. Objectives: Mga Isyung Pangkapaligiran at Pang-EkonomiyaDIANNE BORDANNo ratings yet
- English For Ethiopia: Teacher Guide Grade 10Document12 pagesEnglish For Ethiopia: Teacher Guide Grade 10leta jimaNo ratings yet
- Andrea Kort ResumeDocument1 pageAndrea Kort Resumeapi-513946316No ratings yet
- Newsletter Year 5 Spring Term 2016Document3 pagesNewsletter Year 5 Spring Term 2016DownsellwebNo ratings yet
- Integrated FPDDocument23 pagesIntegrated FPDapi-310655639No ratings yet
- GeneralPhysics1 Q2 Mod5Document28 pagesGeneralPhysics1 Q2 Mod5Jose GulitiwNo ratings yet
- Format Muka Surat HadapanDocument2 pagesFormat Muka Surat HadapanAwang ZulkipliNo ratings yet
- CV Automotive EngineerDocument2 pagesCV Automotive EngineerSohaib RazaNo ratings yet
- Entry Test: ListeningDocument7 pagesEntry Test: Listeningdaya nandNo ratings yet
- Ui V Bonifacio DigestDocument2 pagesUi V Bonifacio DigestPamela Claudio100% (2)
- Project Report On Recruitment Process At HFCLDocument73 pagesProject Report On Recruitment Process At HFCLVarun KumarNo ratings yet