Professional Documents
Culture Documents
Quality Management and Laboratory Accreditation in A Resource Limited Setting
Uploaded by
Ado AbubakarOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Quality Management and Laboratory Accreditation in A Resource Limited Setting
Uploaded by
Ado AbubakarCopyright:
Available Formats
Quality management and Laboratory Accreditation in a Resource Limited Setting:
*AG Abubakar, M Ahmadu, Gideon Tok, O Balogun, A Ojo, I Mamman, N Agala, S Osawe, C , O Oke, T Jelpe, S Peters Institute of Human Virology, 252, Hebert Macaulay Street Central Business district Abuja. *gabubakar@ihvnigeria.org
INTRODUCTION
Medical Laboratories are subject to so many national and international requirements geared towards precise and accurate results for the patients safety. This effort along the line has made it extremely dicult and time consuming to track compliance with every individual organizations listed requirements. Fortunately, the Clinical Laboratories Standards Institute (CLSI) Quality Management Systems (QMS) model provides a means for aggregating all like requirements from dierent regulatory, accreditation, and standards-setting organizations into an easily understandable matrix. This helpful framework allows laboratories to develop quality and technical policies, processes, and procedures that meet all current regulatory requirements. Understanding the modular framework and using it to implement the activities necessary to meet requirements is the laboratorys best and easiest means to build quality into its daily work in the interests of patient care and safety.[1 ] This could be achieved over a good period of time, through training, mentoring and a step wise attitudinal change. Few developing countries have established laboratory quality standards that are affordable and easy to implement and monitor. To address this challenge, the World Health Organization Regional Office for Africa (WHO AFRO) established a stepwise approach, using a 0- to 5-star scale, to the recognition of evolving fulfillment of the ISO 15189 standard rather than an outright pass-fail grading. Laboratories that fail to achieve an assessment score of at least 55% will not be awarded any star ranking. Laboratories that achieve 95% or more will receive a 5-star rating, making them fully prepared for other accreditations. This stepwise approach acknowledges to laboratories where they stand, supports them with a series of evaluations to use to demonstrate improvement, and recognizes and rewards their progress s. WHO AFROs accreditation process is not intended to replace established ISO 15189 accreditation schemes, but rather to provide an interim pathway to the realization of international laboratory standards. Laboratories that demonstrate outstanding performance in the WHO-AFRO process will be strongly encouraged to enroll in an established ISO 15189 accreditation schemes which is affordable, sustainable, effective, and scalable.[2] Recently, this stepwise approach was demonstrated by our laboratory in Jos, Plateau Virology Research Center (PLASVIREC) which tremendously improved from a two star laboratory to a four star laboratory, within just six months. In sub-Saharan Africa in general, and Nigeria in particular, despite the high cost in laboratory testing, aggravated by a slow implementation of the National Health Insurance Scheme, laboratory infrastructure and personnel are adversely affected by a lack of resources and prioritization, hampering laboratory systems in efforts to fulfill their important role in the fight against infectious and chronic diseases. As a result, the accessibility of laboratory testing and the quality of available services remains a serious challenge. It is therefore imperative that laboratory systems be strengthened within broader efforts toward health system strengthening. Efforts to strengthen laboratory systems in the African region have received increased attention in recent years. [2] There is no doubt, in Nigeria that the Presidential Emergency Fund for AIDS Relief (PEFPAR) has been supportive in regard. This article discusses the individual elements of the QMS/WHO-AFRO model and how Nigerian laboratories can use the model to build in a QMS that covers all regulatory and accreditation requirements, prepares laboratories for announced and unannounced inspections, and provides the means for the laboratory to make its best contribution to
patient care and safety. We also made an attempt to provide a step wise approach which will help towards achieving a personnel attitudinal change in the laboratory staff towards building quality into their day to day work.
Laboratory Accreditation and Certification Laboratory certification is a procedure in which a third party gives formal recognition of QMS, most commonly ISO 9001; it does not guaranty the actual technical competence of a laboratory. [36] Accreditation is a formal recognition of technical competence in addition to compliance with QSM. Two key features of accreditation are external review and regular external audits by an external independent body and fulfilling requirement standard, a good example ISO 15189 and ISO 17025.[36] Comparative Advantages of WHO-AFRO Accreditation Gershy-Damet (2010) and others also pointed out that the WHO-AFRO laboratory accreditation process has 4 key comparative advantages: accessibility, affordability, scalability, and sustainability. Like the process itself, these advantages build on each other in a stepwise manner. Accessibility The stepwise approach they described above makes the WHOAFRO accreditation process accessible to public sector laboratories at various levels of development. Rather than deferring participation until the requirements of ISO 15189 are in place, countries can enroll in the WHO-AFRO program now and, through it, track the achievement of their laboratories toward upper-tier status. The WHO-AFRO program benefits countries that lack an established national accreditation body and/or find that the services of international and regional bodies may not yet be easily accessible. Affordability The WHO-AFRO accreditation process is available to countries free of charge, eliminating a critical barrier to enrollment. This enables health officials and policy makers to begin to immediately develop national strategic plans that prioritize accreditation across their laboratory networks without undue financial constraints. To address other key costs encountered in the drive to accreditation, WHO AFRO will provide member countries with free proficiency testing (PT) services from a center currently being established in Senegal, and affordable calibration services are also being developed. These services will complement the WHO-sponsored PT panels currently provided to member countries. Rather than paying for external services, countries should instead dedicate their resources to strengthening laboratory quality systems. Scalability The accessibility and affordability of the program make it scalable for countries in the African region. The stepwise approach and limited cost to the user make it feasible for ministries of health to develop plans that, for example, involve their regional, provincial, and district laboratories in the within a few years. Sustainability Each of the 3 previously described advantages make the WHO-AFRO program a sustainable means for promoting laboratory accreditation. For those minding budgets, afford-ability may be the most important factor in the year-over-year viability of the program. However, the scalability of the program enables the development of vital experience in the operation of laboratories striving toward accreditation across a greater number of laboratories. This will build a broader experience base in the laboratory workforce that will aid the cascade and consolidation of national efforts. This experience base will aid the longer term development of national laboratory experts who can contribute to and lead regional and national accrediting bodies. These advantagesaccessibility, affordability, scalability, and sustainabilityposition the WHO-AFRO laboratory
accreditation process to have a marked influence on improving the quality of laboratory systems in the African region during the next 5 years.
Building Blocks of the Accreditation Process There are several key building blocks of the accreditation process: (1) the role of WHO AFRO, (2) standards and assessment tools, (3) assessors and assessor training, (4) equipment calibration and biosafety, (5) laboratory management training, and (6) a PT provider. The Role of WHO AFRO Few countries in Africa have their own accrediting body for ISO 15189. Although not an accrediting body, WHO AFRO has established this stepwise accreditation process for medical laboratories in accordance with the WHO mandate to develop, establish, and promote international standards with respect to food, biological, pharmaceutical, and similar products and the WHO AFRO efforts to strengthen the tiered laboratory systems of its member states. In this capacity, WHO has accredited laboratories for important diseases, including polio, measles, and influenza, and HIV drug resistance monitoring. Accreditation will be a crucial capacity-building focus of the WHO AFROsupported Laboratory Network. The governance structure of the WHO-AFRO Laboratory Network includes a technical advisory group on laboratories that will provide oversight of the accreditation process and advise the WHO-AFRO secretariat on laboratory capacity building in the African region. Standards and Assessment Tools The WHO-AFRO laboratory accreditation process is based on ISO standard 15189:2007(E). The process is accessible to ministries of health for all laboratories providing clinical testing services. The accreditation checklist is organized into headings similar to the Clinical and Laboratory Standards Institute Quality Systems Essentials. These 12 areas of assessment cut across both sections of the ISO 15189 standard (management and technical requirements) and help to facilitate the inspection process .The accreditation checklist evaluates areas common to ISO 15189 and other laboratory standards, such as ISO 17025, the evaluation criteria of the CAP, and the standards Thailands Medical Technology Council developed for use in Thailand . The checklists 12 sections provide assessment on the basis of 110 clauses and 250 total possible points. Each item has been assigned a weighted value of 2, 3, or 5 points based on complexity and/or relative importance. Incomplete fulfillment of an item can be scored as partial and awarded a single point, with written explanation. Some clauses in the checklist are tick lists and require the satisfactory presence of all subitems listed below the main heading to receive full credit. Baseline assessments using the WHO-AFRO checklist can be analyzed and presented as a gap analysis for national accreditation efforts, revealing facility-specific challenges and systemic areas of need that must be prioritized and addressed. Over time, progress in strengthening laboratories can be tracked by comparing assessment findings. In Lesotho, the WHO-AFRO checklist has been used as a monitoring tool to evaluate laboratories receiving mentoring support; these assessments have already helped to quantify and demonstrate areas of laudable progress and continuing challenge. Assessors and Assessor Training Accreditation will be awarded based on biannual assessments of laboratories conducted by assessors selected and trained by WHO AFRO. These assessors will be drawn from laboratories across sub-Saharan Africa. Assessors are being trained in 2 training centers, one in Kenya for English-speaking assessors, and the other in Cameroon for Frenchspeaking assessors. Assessor teams will be led by a team leader, and their size and composition will vary based on the scope of the laboratory seeking accreditation. Assessors will not be permitted to assess laboratories in their country of residence and will not be financially compensated.
Calibration and Biosafety
WHO AFRO, in close collaboration with the African Field Epidemiology Network Laboratory in Kampala, Uganda, will provide training on equipment calibration and biosafety for countries engaged in the accreditation process. Assessment Section Documents and records Management reviews Organization and personnel Client management and customer service Equipment Internal audit Purchasing and inventory Information management Process control and internal/external quality assessment Corrective action Occurrence/incident management and process improvement Facilities and safety Points 25 12 20 8 30 10 30 14 43
Table Health for Africa Points for Section
1.Sections of the World Organization Regional Office Accreditation Checklist and Each
8 10 40
Total
250
Laboratory Management Training and Mentoring Strengthening Laboratory Management Toward Accreditation (SLMTA) is an innovative task- and competency-based training and mentoring tool kit jointly developed by the CDC, WHO AFRO, the Clinton Health Access Initiative, and the American Society for Clinical Pathology that equips laboratory managers preparing for accreditation. SLMTA begins with baseline assessments with the WHO-AFRO checklist and uses a multiple workshop model with supervised improvement projects conducted between trainings. A series of training sessions has been held at the African Center for Integrated Laboratory Training at the National Institute for Communicable Diseases, Johannesburg, South Africa, to build national training teams for SLMTA in 12 countries including Nigeria (with 12 trained assessors). Laboratory mentors who spend extended well-structured periods embedded in the daily life of a laboratory are also a valuable means of accelerating a laboratorys path toward accreditation. The SLMTA training tool kit is well suited for use by mentors in facility-level work. Proficiency Testing
The Department of Bacteriology and Virology of the Dantec Hospital, Dakar; Digital PT, Westford, MA; National Institute for Communicable Diseases; and National Health Laboratory Services, South Africa, will provide comprehensive PT for several analytes, including serology, microbiology, chemistry, hematology, and parasitological testing. The accreditation process will also accept PT programs by other recognized providers.[2] In Nigeria, some implementing partners and the Medical Laboratory Council are preparing PT panels for hematology, CD4, blood chemistry and rapid testing.
Table2. Some External Quality Assurance programs currently in Nigeria Organizing Agency Axios Type of activity Supporting PT panels distribution from South Africa PT Intervals Monthly and bimonthly Twice a year Specialties covered HIV serology and CD4 Haematology, chemistry, HIV serology HIV Serology, Haematology, chemistry,CD4, TB smear HIV-1 DNA DBS Influenza Molecular Diagnosis Number of Laboratories Involved 81 and 64 respectively 1,400
MLSCN
IHVN
PT
Quarterly
76
CDC WHO/EQUAP Japan
PT(Atlanta) Retesting (Nigeria) PT
Quarterly Once a year Twice a year
18 1
Specific Criteria: In addition to the 12-section, 250-point assessment checklist, several specific criteria are required to receive recognition in the WHO-AFRO accreditation process.
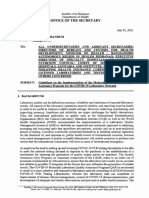
The WHO-AFRO Stepwise Accreditation Approach Recognizing the gap between the current state of laboratories and the requirements of ISO 15189, the WHO-AFRO approach provides laboratories with stepwise recognition of evolving fulfillment of the ISO 15189 standard rather than binary pass-fail grading. This program is not intended to replace established ISO 15189 accreditation schemes, but rather to provide an interim pathway for measuring, monitoring, and recognizing improvement toward the realization of international laboratory standards and subsequent application to full ISO 15189 schemes. The WHO-AFRO accreditation process provides a framework to establish an effective quality management system for medical laboratory testing, characterized by strong programs for quality assurance, quality control, and quality improvement. All testing areas and processes are included, from pre-analytical through post-analytical procedures, as are laboratory safety and ethics. Following assessment, laboratories will be recognized on a 0- to 5-star ascending scale. Laboratories that fail to achieve at least 55% on assessment will not be awarded a star ranking. Laboratories that achieve 95% or more will receive a 5-
star rating Figure1 below. Once assessed, laboratories are expected to maintain their star status and work toward the next star. Laboratories awarded 5 stars will be strongly encouraged to enroll in an established ISO 15189 accreditation scheme. This stepwise approach acknowledges laboratories where they stand, supports them with a series of assessment opportunities, and recognizes and rewards progress over time. The WHO-AFRO program benchmarks current performance, evaluates the distance remaining to achieve international standards, and establishes a mechanism for tracking progress toward these goals. Technical support
will be intensified by AFRO and partners to help countries meet their accreditation goals. The program is expected to have a catalytic effect, encouraging the incorporation of accreditation goals into national strategic and operational plans, sensitizing policy makers and laboratory staff on accreditation, and nurturing the development of laboratories in the African region.
Figure 1. World Health Organization (WHO) Regional Office for Africa (AFRO) accreditation scheme showing the stepwise recognition of laboratory performance. Based on the percentage score, laboratories are assigned an accreditation level, based on 1 to 5 stars. Laboratories that receive a 5-star rating are strongly encouraged to transition to an internationally established accreditation scheme. The purpose of the WHO-AFRO accreditation is not to replace CAP, ISO, SANAS, or SADCAS accreditation, but to serve as an accreditation scheme to assist the laboratories in obtaining these internationally recognized accreditation standards. CAP, College of American Pathologists; ISO, International Organization for Standardization; JCI, Joint Commission International; SADCAS, South African Development Community Accreditation Service; SANAS, South African National Accreditation System
Clinical Laboratories Standards Institute (CLIS) simple model for a laboratory quality system: As mentioned earlier, Laboratories that have attained the 5 star grading are encouraged to enroll for ISO 15189. The CLIS, model is pertinent to achieving this goal. Medical laboratory work is composed of the technical activities that produce laboratory results for patient care and the management activities that support the technical work. It is the job of the laboratory technical sta to perform pre-analytic activities (blood sample collection, receiving, accessioning); analytic activities (testing, examinations, interpretation); and post-analytic activities (reporting results, archiving samples, charge capture) that transform a clinicians request for a laboratory test or examination into the results used by the clinician to diagnose and treat patients. Likewise, it is the job of the laboratory supervisory and managerial sta to design and implement the supportive infrastructure that is necessary for the technical work to proceed unimpeded. A good team work between technical and managerial activities is essential for the continuous, unimpeded realization of highquality, error-free, ecient, and eective laboratory operations. Fig. 2 depicts this important relationship between technical and managerial activities. Importantly, this gure also represents a QMS model that can be used in the medical laboratory environment.[1,33]
Quality
System Essentials (QSEs)
Documents and Records Organization Personnel Equipment Purchasing and Inventory Process Control Information Management Occurrence Management Assessment: External and Internal Process Improvement Customer Service and Satisfaction Facilities and Safety
Fig. 2. A simple generic model for a quality management system (From CLSI. CLSI approved guideline HS1: a quality system model for health care. 2nd edition. Wayne (PA): 2004. p. 4
Implementing a quality management system: Most laboratories are already performing management activities that comprise components of a QMS. Without a standardized QMS in place, however, not all necessary management activities are practiced in every laboratory and those that are may not be practiced uniformly within a single laboratory. The resulting variation in management practice causes ineciencies in the use of resources and ineectiveness in meeting accreditation and regulatory requirements. The QMS is a uniform, systematic means for any laboratory to ensure that requirements are being continuously met each time, every time, in every laboratory section, every day. Before a new testing can be performed, laboratory management must implement a number of critical infrastructural elements in a logical sequence and ensure they are solidly in place. First, the specic pre-analytic, analytic, and post-analytic work processes and procedures for the new testing need to be identied. Next, the laboratory must determine the responsibilities and reporting relationships of all the people involved in the new service. Then, it needs to identify its potential customers and determine their needs and expectations for the new service. Next, adequate facilities, people, equipment, and materials need to be identied, sought, obtained, and put in place for the new service. The specic pre-analytic, analytic, and post-analytic work processes and procedures need to be developed, validated, and documented. Sta needs to be trained and their initial competence assessed. The laboratory needs to determine the means by which patient results and reports will be managed for
the new service. There is need to determine the laboratorys means for capturing complaints and non-conformances for the new service. The laboratory needs to determine how it will measure its performance to determine if goals, objectives, and customer expectations are being met for the new service. The laboratory needs to determine the means by which quality reports will be periodically prepared for the new service. Last, the laboratory needs to determine how management will review and identify opportunities for process improvement and prioritize and initiate improvement activities.
Only after all these elements are nally in place and functioning, may the new service testing nally begin. One way to depict this important sequence of managerial events is by slightly modifying the QMS model as rst shown in Fig1. This modication is shown in Fig. 2 which depicts the QSEs as divided into three groups: (1) laboratory, (2) work, and (3) measurements. These three groups sequentially embody the entire laboratory as a dynamic, whole organization. Every essential component needs to be in place for the laboratory to create and maintain its complete structural integrity. The laboratory can implement its entire QMS by establishing the policies, processes, and procedures for the QSEs shown in Fig. 3, following the prescribed sequence of the three groupings.
Fig. 3. Arrangement of the quality system essentials of the QMS model into logical groupings. (Adapted from CLSI. CLSI approved guideline HS1: a quality system model for health care. 2nd edition. Wayne (PA): 2004; with permission.)
This sequential approach is also eective when planning any new laboratory service, or when regionalizing any two or more laboratories within the same health system, or when creating a new entity through mergers. To clarify the QMS sequential model further, the elements of each QSE are individually described next. Each element represents a laboratory requirement, as specied by regulatory agencies, accreditation organizations, or in published standards. The laboratory quality system essentials Organization The laboratory needs to be legally identiable and have a documented organizational plan and structure that ensures the delivery of quality services to patients and all clinical personnel responsible for patient care and ensures patient safety.[3] This plan and structure should include: Scope Roles, responsibilities, and reporting relationships Quality planning and risk assessment Budgeting of resources Quality review and assessment Management review
The scope of all of the laboratorys services should be clearly documented, with a description of all testing services provided and all customers served. All personnel roles, responsibilities, and reporting relationships need to be documented and communicated so that all sta members are aware of their respective places in the organization. Quality planning and risk assessment should be undertaken to ensure that all applicable accreditation and regulatory requirements are met with the laboratorys current, modied, or new processes and procedures. Allocation (ie, budgeting) of facility, human, equipment, and material resources is necessary for ensuring that resources provide adequate capability to meet customer needs. A QMS requirement is that laboratory management periodically reviews the eectiveness of the QMS in meeting customer needs, stated goals and objectives, and applicable requirements [12,1618]. This last activity, management review, should culminate in the laboratorys prioritization of opportunities for improvement, allocation of resources to carry out the improvements, and monitoring of improvement activities to ensure their eectiveness. Facilities and safety The laboratory needs to have adequate space and facilities that are designed and constructed or renovated to optimize work eciency; minimize the risk of injury and occupational illness; protect workers, visitors, and patients from recognized hazards; and meet governmental or industry standards for facilities and environment. Listed next are several structural and nonstructural elements of laboratory design that aect the planning, layout, and safety of the laboratory [19].
Space Workow Casework Equipment placement Classications Ventilation Lighting Plumbing Electrical Communications
Arrangements are needed for routine maintenance to keep the facility in a functional, reliable, and safe condition. Ensuring clean work areas and good housekeeping involves laboratory sta and ancillary services provided by the larger organization. The laboratory should have adequate space for storage of consumable supplies; reagents and chemicals; patient samples; and materials derived from patient samples, such as tissue blocks and retained slides. Physical and procedural safety is an inseparable adjunct to the physical facility. Several safety programs that are required in the laboratory are Emergency preparedness (re, weather, disaster) Universal precautions [20] Hazardous waste [21] Chemical hygiene [20] Infection control [22] Occupational injury and illness [20,23] Radiation safety (where applicable) [13,24] Ergonomics [17]
Supportive safety training is required in each respective program for each sta member as is applicable to his or her respective job tasks. Personnel Once the organization structure and responsibilities have been established and the laboratorys physical space needs have been addressed, the laboratorys personnel is the next important resource to be established. Certainly, without qualied, trained, and competent sta performing the work processes, quality laboratory performance cannot be ensured. The Clinical Laboratory Improvement Amendments of 1988 regulation [25] species the minimum requirements for the qualications and responsibilities for personnel performing provider-performed, moderate-complexity, and high-complexity laboratory testing. The job titles for which these national personnel standards exist are shown in Table 2.
Laboratories and their parent organizations may set additional or higher qualications and responsibilities, if so desired. Qualications and responsibilities for the laboratory director, consulting pathologists, and technical consultants (for which the laboratory is assessed at its periodic unannounced inspections) have been published by the College of American Pathologists [26]. All personnel qualications and responsibilities can be documented in the laboratorys job descriptions, which must be kept current and available to all sta. The laboratory should provide an induction for all new laboratory sta. Suggested elements for laboratory orientation are as follows: Laboratory quality policy Laboratorys vision and mission Laboratory values Laboratory goals and objectives Personnel qualications and responsibilities Laboratory culture
All sta needs training in the work processes and procedures that comprise their respective job tasks, whether or not new sta members arrive with previous experience. The required ways to ensure that competence of sta is assessed and documented initially after training and periodically thereafter are listed as follows [17,25]: Direct observation of routine work processes and procedures Direct observation of equipment maintenance and function checks Monitoring the recording and reporting of test results Review of work records Assessment of problem solving skills Use of specially provided samples, such as those from previously tested patients, inter-laboratory comparison materials, or split samples. Table 3. Job titles for which there are Clinical Laboratory Improvement Amendments of 1988 personnel standards
Provider-performed microscopy Laboratory director Testing personnel
Moderate-complexity testing Laboratory director Technical consultant Clinical consultant Testing personnel
High-complexity testing Laboratory director Technical supervisor Clinical consultant General supervisor Testing personnel Cytology general supervisor Cytotechnologist
To ensure that laboratory sta remains current in job and professional knowledge, laboratories are required to provide programs for continuing education and professional development [12,17]. Records of the laboratorys continuing education program are required. Records of personnel participation in internal and external continuing education and development should be maintained in personnel les. In addition to the processes described previously, laboratory sta must also collaborate with the parent organizations human resources department for other required activities, such as occupational immunizations, accident reporting, and wage and payroll registration. Equipment Once the laboratorys organization, facility, and personnel are in place, the laboratory needs to acquire the equipment necessary for delivering its desired testing services. The processes, programs, and procedures described for this QSE refer to the laboratorys general equipment, instruments and analytical systems, and computer systems hardware and software. The laboratory should establish selection criteria for each piece of equipment it needs to acquire, and should determine which vendors can meet those criteria. Before equipment is selected, the laboratory needs to verify that the laboratorys physical facility can meet the equipments needs for space and load bearing; electricity, ventilation, humidity, and temperature; water type and quality; and any other special requirements. After arrival, and before use, each piece of equipment needs to be installed and initially veried as meeting the manufacturers stated performance characteristics. After the onset of the actual testing, the equipment must also be veried as functioning as intended in the actual work processes in which it is used. Laboratory schedules and procedures that follow manufacturers instructions are required for ongoing preventive maintenance, calibrations, and calibration verication; performance records provide objective evidence of outcomes of these required activities. Troubleshooting, service, and repair records are also required. Reconstruction of the history of each piece of equipment from acquisition to decommission should be traceable from the equipment records. Purchasing and inventory Before any testing in any new laboratory or new process can begin, the laboratory needs to identify and purchase all related materials and reagents. The laboratory may also need to purchase services, such as equipment maintenance and service contracts and referral laboratory testing. For these purposes, the laboratory should formalize its needs and requirements in documented agreements with vendors that specify each partys responsibilities. These agreements should be periodically reviewed to determine the vendors ability to meet the laboratorys needs, and adjusted as necessary.
Ecient laboratory operations require the uninterrupted availability of reagents, supplies, and services. The laboratory needs to maintain a cost-effective disposable supply inventory and have the support of an adequate materials purchasing program. Critical reagents and materials need to be received, evaluated, and tested as necessary (before use) to ensure that necessary quality requirements have been fullled. The work quality system essentials Process control Control of the laboratorys pre-analytic, analytic, and post-analytic work processes is crucial to the quality of the laboratorys test results. Such process control begins with identifying and documenting the laboratorys many work operations. A concise guide of laboratory processes with examples is available [3]. Use of properly constructed process owcharts eciently identies the activities for which procedures (ie, instructions) are needed for the laboratory sta to perform their assigned job tasks. Such process analysis expedites the writing of individual procedure documents. Together, the process and procedure documents conveniently form the basis of the technical procedures manuals. Before any process is executed in the live environment, the process needs to be veried as meeting its intended outcome. Verication consists of creating a plan that allows the technical sta to challenge the process as initially developed, document the results, and determine if the pre-established criteria set for the process have been met and whether the needs of the customers of the process have been met. In processes where laboratory testing is performed, test method verication is also required. Also, the laboratory must verify that the manufacturers stated specications are being met with the laboratorys own processes, equipment, personnel, and materials. Several guidelines are available to assist laboratories in such verication of test methods. Quality control programs are a means of controlling patient testing processes at the bench level. Laboratories must meet the established requirements for quality control of test methods; both the minimum required quality control [14] and any manufacturers requirements must be followed. The use of statistical tools provides a visual means to understand quality control data so that timely action can be taken when method problems are detected [6]. Documents and records At the heart of the laboratorys QMS are the policy, process, and procedure documents that tell sta what to do and how to do it and the records that provide objective evidence of the results of performing the processes and procedures. Audits often reveal that laboratory documents and records are missing, incomplete, outdated, or contain incorrect information; all these problems can cause errors that could compromise patient safety. Laboratories are now required to control their documents and records through the processes listed next [6,8,9]:
Document control elements Document identication Creation, review, and approval of new documents Document master les Review and approval of changes to approved documents Periodic review of unchanged documents Master index of documents Document distribution Archiving, storage, and retention of obsolete documents Record control elements Record identication Creation and legibility Records reviews Record indexing Records access Changes to recorded information Record storage and retention Record disposal Either or both paper or electronic document control systems are acceptable, provided that only the most current documents are available to all sta at the locations where they are needed for sta to perform their assigned job tasks. Information management The requirements contained in this QSE concern the laboratorys management of the information contained in its paper-based or computer-based record systems. This includes patient demographics, test results and interpretations, reports, other laboratory data and information, and how that information is disseminated to users or other computer systems. The laboratory needs to have policies, processes, and procedures that address information access and security; requests for information; condentiality of information; information transfer (eg, electronic interfaces and data transfer); and data integrity (eg, report readability and accuracy). Also, there needs to be a downtime program for managing the availability of patient results and information when the computer system is not functioning. In addition, this QSE contains the requirements for the processes to ensure against Medicare and Medicaid charging and billing fraud and abuse [36].
The measurement quality system essentials Up to this point, eight QSEs (presented in sequential terms of laboratory and work) have described the actions needed to prepare for the laboratorys production of testing and examination result reports. The remaining four measurement QSEs shift the focus to asking and answering the question of how well the laboratorys processes are performing in meeting the quality goals and objectives set in QSE: Organization, the requirements imposed by regulatory agencies and accreditation organizations, and the needs of the laboratorys customers. These are the QSEs of measurement. Occurrence management Now referred to as nonconforming event management, this QSE consists of the requirements for documenting and investigating events that do not conform to the laboratorys established policies, processes, or procedures, or other imposed requirements. The program captures and analyzes information about nonconforming events and complaints to identify underlying systematic problems and gain managements commitment to removing the causes. A nonconforming event management program contains the following elements [37]: Identication and reporting Remedial action Investigation and documenting Action plan Classication Analysis and presentation Management review and follow-up
This QSE also includes the recently established requirement for the laboratory to have a process for employees to communicate concerns about quality and safety to laboratory management [17]. Assessments: external and internal The laboratory cannot improve the quality of its services without measuring its current performance. Both external and internal assessments provide objective evidence of the laboratorys performance compared with established goals. The laboratory should be participating in three types of external assessments: (1) licensing or accreditation, (2) prociency testing, and (3) performance comparison. First, all laboratories are subject to external assessment by licensing agencies (eg, Centers for Medicare and Medicaid Services, under the Clinical Laboratory Improvement Amendments of 1988) or accreditation organizations, such as the Joint Commission, College of American Pathologists, or Commission on Oce Laboratory Accreditation. These organizations assess the laboratory against their respective published requirements and issue deciencies for identied nonconformances that require subsequent corrective action for the laboratory to maintain the license or accreditation.
The second type of external assessment is prociency testing, where the laboratory tests or examines sample materials prepared and sent by an outside organization, the results of which are compared with other laboratories with similar methods and instrumentation [25]. The third type of external assessment involves the laboratorys comparison of its performance on selected process measurements against other laboratories of similar size and scope. The College of American Pathologists maintains two such programs: Q-PROBES and Q-TRACKS [38]. Routinely, laboratories should practice two types of internal assessments: quality indicator measurements and laboratory audits. Quality indicators are measurements of process performance that are tracked using graphical tools, such as control charts. One example is the number and source of received samples that do not meet the laboratorys established acceptance criteria; another is turnaround time. Ideally, the laboratory identies one or more indicators to measure the performance of its pre analytic, analytic, and post analytic work processes. Many examples of laboratory indicators are available [10, 17]. A laboratory audit is the process of comparing observations of actual conditions with requirements and presenting an evaluation of the results to management [40]. In the laboratory environment, any pre analytic, analytic, post analytic, or management process can be audited to determine its conformance to the laboratorys established policies, processes, and procedures, and external regulatory and accreditation requirements. College of American Pathologists inspectors are using (vertical) auditing techniques to follow the sample through the laboratorys processes during unannounced laboratory inspections [17]. Audit ndings point to process problems that need corrective action. Customer service The laboratory provides phlebotomy services to patient customers and provides test results, interpretations, and reports to its clinical caregiver customers. Adequate measurement and monitoring of laboratory performance requires feedback being actively, routinely solicited from these customers regarding their satisfaction with the laboratory services they have received [17]. Suggestion box, questionnaires, records of clinical meetings is good examples of what a good assessor will look out for under customer satisfaction. Also, laboratories that perform referral testing have other laboratories as external customers. The referral laboratory should routinely assess these other laboratory customers satisfaction with its referral services that includes the performance of any couriers, call centers, and reports involved. The satisfaction of the laboratorys internal (employee) customers should also be periodically assessed, with feedback provided.
Process improvement Measurement and monitoring of laboratory process performance points to opportunities for improvement. All measurement activities, such as quality control, prociency testing, nonconforming events, external assessments, internal quality indicators, performance comparisons, quality audits, and customer satisfaction feedback provide information that points to pre analytic, analytic, and post analytic processes that are currently problematic or have the potential to become problematic if no preventive action is taken. The laboratory needs to prepare information from measurement activities into a periodic report that is reviewed by laboratory management, with prioritization of problems for improvement and allocation of resources for these improvements. Improvement teams should be convened and assigned to specic problems for solution. Several dierent quality tools are available for determining the root cause of the problems and identifying potential solutions. Quality tools from the nonmedical manufacturing arena have been adapted to improve health care processes, including Failure Modes and Eects Analysis, Lean, and Six Sigma: Failure Modes and Eects Analysis is a tool used to analyze the activities in a process for points of vulnerability, potential and actual risks, or failures. Scores for likelihood of failure detection, probability of occurrence, and severity of outcome are assigned, calculated, and prioritized. Process adjustments are made to reduce or remove the risks and improve the outcome. This process needs a lot technical expertise, team work between the laboratory and clinical groups and everybody has at an alert for reviews. Lean is a work philosophy that strives to eliminate waste from a process, rst practiced and then formalized into the Toyota Production System [19]. Medical device manufacturers and industry consultants now oer Lean consulting services because many laboratories realize that a more ecient throughput means an increase in the laboratorys capability for more testing, often without additional resources [20-23]. Lean tools and principles are also being actively applied to eliminate delays, overcrowding, and frustration associated with the existing health care system [24]. While this approach sounds good to the mangers and employers of services in cost cutting, care has to be taken not to compromise professionalism, specialization and thrive for excellence. Six Sigma is a methodology that uses proved quality principles and techniques to reduce process variation and decrease errors toward the 6s level of 3.4 defects per million opportunities, so that compliance with requirements and with factors critical to customer satisfaction can be achieved [25]. The ve major activities of any Six Sigma project (dene, measure, analyze, improve, and control) include measurements, statistical analysis, and tracking to tie together quality, cost, processes, people, and accountability. Six Sigma methodologies have been successfully applied in the automated laboratory environment [26] and to health care in general [27]. Comparisons of error rates for selected laboratory pre-analytic, analytic, and post-analytic processes demonstrate that laboratory processes have yet to achieve the Six Sigma goal [28, 29]. This method will surely work with realities on ground and will keep all hands on deck towards achieving zero tolerance to error in clinical laboratories.
Combinations of Lean and Six Sigma methods have been applied to both health care processes and the medical laboratory [30,31]. Applications of this subject continue to grow, as reported in health care journals, laboratory periodicals, and Internet reports. Numerous opportunities for individuals to become certied in Lean and Six Sigma methods are available for laboratorians so interested; an Internet search provides ample information.
Incremental quality tools versus systematic quality management The 12 QSEs comprise a systematic approach to quality management that ensures the laboratory meets all applicable requirements as part of performing everyday pre-analytic, analytic, and post-analytic activities. Unfortunately, there is a pervading assumption that Failure Modes and Eects Analysis, Lean, and Six Sigma alone solve the quality problems of both laboratory and health care services. These, however, are merely single tools for improving only one work process at a time. These three tools can also, and should be, applied in QSE process control when the laboratory develops a new process (eg, the example of adding a new testing service to diagnostic testing). Most laboratories use these quality tools only for identied problems, however, thereby missing the opportunity to have initially designed, documented, validated, and implemented the processes optimally to identify any and all problems that actually arise, before implementation. Likewise, none of the Total Quality Management, continuous Quality Improvement, and Plan-Do-Check-Act programs popular in the 1990s has solved the problems of medical errors causing patient injury and death so clearly documented in recent history. It can be argued that the reason for these failures has not been within the tools themselves (used properly, the aforementioned tools do indeed eect improvements) but rather that these tools have been used in isolation, instead of being incorporated into a system for quality. What many laboratories lack is a fundamental foundational approach to quality in which the desired level of quality and process performance are built into each laboratory process such that [32,33] All applicable requirements and customer needs are met the rst time, every time. Measurement and monitoring activities provide objective evidence of process performance. Laboratory management actively reviews reports of process performance. Laboratory management takes visible, denable actions to remove root causes.
The approach that most successfully integrates all regulatory and accreditation requirements, customer considerations, patient safety, process design, measurement, monitoring, and improvement is that of implementing a QMS, such as the previously described 12-QSE model, which supports the laboratorys entire path of pre-analytic, analytic, and post-analytic workow. This model is generic and applicable to laboratories of any size, scope, or specialty anywhere in the world. It has also been deemed simple enough to have been adapted for use in African countries supported by the Presidents Emergency Program for AIDS Relief [4]. A number of United States and Canadian laboratories have successfully used the model for implementing quality management as a means to achieve process improvement and patient safety and readiness for unannounced laboratory inspections. These laboratories have reported signicant decreases in the numbers of deciencies found during accreditation inspections and decreases in the cost of process failures, such as errors made at sample receiving (Sutter Health Sacrament-Sierra region and University of Alberta, Edmonton, personal communications, May 2007). pSMILE - (Patient Safety Monitoring & International Laboratory Evaluation) has been supportive to many developing countries.[37]
Sustaining a culture of quality in the medical laboratory From all accounts in the nonmedical industry, quality literature, and all testimonials of Malcolm Baldrige award-winning organizations, leadership is the key ingredient in organizational quality improvement. Leadership sets the tone and culture for quality in any organization. Sta looks to leadership for guidance and follow-through and, lacking either, quality becomes relegated to the minimum required practice.[14] Two types of leadership exist in most laboratories: medical leadership and scientific leadership. Both are needed to support a sustainable culture of quality management in the medical laboratory environment. Laboratory scientific/administrative management should focus on setting the policies, processes, and procedures for the QSEs, removing barriers that prevent sta from getting their respective tasks accomplished eciently and eectively. The equally important role of the pathologist medical partnership/leadership is to ensure that the policies, processes, and procedures for the pre-analytic, analytic, and post-analytic work ow meet technical requirements and produce clinically relevant, accurate results and interpretations to the laboratorys customers for the purposes of patient care. There is a lot of work for the pathologists which include point of care testing, interpretation of laboratory results to clinicians, buffering the gap between scientists and physicians for instance establishing precise and accurate determination of reference values, critical values and management of pathological conditions of the patients to mention but a few. QSE and path of workow activities require the constant collaboration of both scientific and medical leadership. The QMS model described in this article provides the roadmap in which this collaboration can successfully provide the laboratorys best contribution to patient care and safety.
Management review: According to the accreditation standards, laboratory management shall review the QMS to ensure continuing suitability and effectiveness in support of patient care and to introduce any necessary changes or improvements. The results of the review shall be incorporated into a plan that includes goals, objectives and action plans (ISO 15189, 4.15.1). Emphasis should be on developing an overview of the many elements of a QMS, such as the results of IQC, EQA, internal audits and external audits, previous MRs, quality indicators, turnaround times, status of preventive and corrective actions, NCs, complaints, feedback and evaluation of suppliers. Questions to be asked (and answered) include the following: Do we still support our objectives and quality vision? and Are we still satised about the way certain elements of the QMS are implemented? The management should dare to change directions or lower criteria when initial objectives are too ambitious, but they should still aim for continuous improvement. The standard states that an MR typically occurs once every 12 months. However, in some laboratories, it may be more efcient to perform segmental MRs, ensuring that by the end of the year all elements are
tackled. As the information discussed during the MR is extensive, a good preparation is essential. The whole process is driven by the management, but they can delegate tasks to the quality manager to collect all the data, decide what needs to be discussed and how the data will be presented. In other words, he or she denes the agenda, invites the participants of the meeting (management or staff and usually the quality team members) and contacts the people in the laboratory responsible for collecting the necessary data summarized above, which form the input of the MR. Usually, the quality manager or laboratory director chairs the MR, but is not the only person who talks. One way to prepare for the meeting efciently is to have a meeting in advance with all the people who will collect data, or at least share a template ahead of time, to standardize the way the results are presented by different groups.
Collected data are then provided to the management before the meeting in a structured manner. This leads to an MR meeting focused on the right topics, nished within a reasonable time. Difcult or technical subtopics could be addressed in a separate meeting with fewer participants. The outcome of the MR should include an action plan (what, who and by when?) and the objectives of the next year, leading to a continuous improvement for the patients. In addition, resource needs or important decisions could be enclosed.
All this information should be written in a report that is absolutely necessary, as it is a way of registering your quality. The report is dated and signed or approved afterwards. The quality manager is responsible for the follow-up of the action plan. All laboratory staff is informed of the results of the review. Quality indicators are important input elements used in an MR. The standard mentions that Laboratory management shall implement quality indicators for systematically monitoring and evaluating the laboratorys contribution to patient care. When this program identies opportunities for improvement, laboratory management shall address them regardless of where they occur (ISO 15189, 4.12.4). To facilitate a successful MR, the techniques of motivation and change management (see further) could be applied. Use a logical structure, in an understandable and meaningful way, to present the information. Start with some positive elements, show solutions, but keep focus and respect the timing. Consider the audience and adjust the content of the presentations to suit them. Listen actively and verify that everybody understands and agrees. Finally, an MR is a process in which the whole laboratory is involved, not only management and the quality manager. All people working in the laboratory can help to collect data where appropriate, and should be informed about the outcome and the action plan.
Human side of change processes
One of the biggest challenges in implementing QS in the laboratory lies in overcoming the natural reluctance of team members and convincing them of the value of QAu to justify the effort that will be required. Implementing a specic change in the laboratory is a linear process. For example, the head of the laboratory decides, together with his staff members, to implement QS. The different steps (writing SOPs, tracking NCs and so on) and when they should be implemented is denable. This linear process is usually organized with the help of techniques such as project management and is restricted in time. However, the behavioural change the reaction of Scientists in the laboratory cannot be planned in time, as it is a cyclic process. The scientists will go through a learning process, during which they receive new information, experience certain emotions try out new things and adapt to and integrate their knowledge. This process differs between individuals and cannot be managed in the same linear manner. Tension will emerge between those two processes and this will cause resistance during a change process. This resistance cannot be avoided, but when managed well, can increase the effectiveness and efciency of the change you would like to implement. The cyclic process mentioned above encloses different phases people may go through when confronted with change, as described by KublerRoss. [36]
Initially, people tend to deny the impending change and continue with their work. They progressively become aware that the change is signicant and may begin to doubt and become angry. Consequently, people will negotiate and try to maintain the status quo. When it is accepted that change is inevitable, they may become depressed. After a period of inner struggle, people see new opportunities, start exploring them and develop alternatives to go about with the changes. In the last phase, they accept the situation and plans can be made to continue. Each individual will go through these phases, but at different speeds, resulting in the need for exibility, in particular from the management. In an attempt to implement change, first, patiently repeat the message and the facts to people in the shock and denial phase. Second, give them the opportunity to blow off some steam and listen. If they start to negotiate, be rm, which can be followed by encouragement. Once people accept what is going to happen, do not minimize their efforts and be positive. A useful tool to help navigate more efciently through the whole change process is force eld analysis, which helps to traverse the phases of change in a participative way with your team or department (group problemsolving tool). The underlying concept is that every situation involves a balance between conicting forces, driving forces and restraining forces. Driving forces (or enablers) are actions, skills, equipment, procedures, people and other factors that help to move towards the desired objectives, whereas restraining forces (disablers) inhibit you from reaching the goals. Force eld analysis is usefully carried out as a group exercise, involving the identication of different forces together. The forces can be prioritized and appropriate actions should be dened to minimize disablers and stimulate enablers so that change becomes possible.
Fig.4 seven elements that influence change readiness
Fig.4 seven elements that influence change readiness Fig.4 seven elements that influence change readiness
Fig.4 seven elements that influence change readiness
CONCLUSION: Recently, the council has opened new positions including that of director accreditation and regulatory affairs this is in addition to its collaboration with the various donor agencies and implementing partners in Nigeria. The USG laboratory technical working group has been supportive. The Medical Laboratory Science Council of Nigeria has a lot to put in place towards local accreditation of laboratories in Nigeria. This will surely assist the laboratories in Nigeria in smoothly scaling through international accreditations. Beyond accreditation is a continuous quality improvement towards a sustainable patient care and safety in Nigeria.
References: [1] Berte, LM. Laboratory Quality Management: A Roadmap Clin Lab Med 27 (2007) 771790 [2] Gershy-Damet G. The World Health Organization African Region Laboratory Accreditation Process: Improving the Quality of Laboratory Systems in the African Region Am J Clin Pathol 2010;134:393-400 [3] CLSI [Formerly NCCLS]. CLSI document GP26dApplication of a quality system model to laboratory services; approved guideline. 3rd edition. Wayne (PA): Clinical and Laboratory Standards Institute; 2004 [4] Available at: http://enews.clsi.org/clsi/issues/2007-04-01/3.html. Accessed on May 15, 2007. [5] Occupational Safety and Health Administration. Code of Federal Regulations, Title 29, Part 1910. Washington DC: U.S. Government Printing Oce, published annually. [6] ISO. ISO standard 15189: Medical laboratories Particular requirements for quality and competence. Geneva, Switzerland: International Organization for Standardization; 2003. [7] ISO. ISO standard 9001: Quality management systems requirements. Geneva, Switzerland: International Organization for Standardization; 2001. [8] Laboratory Accreditation Program. Laboratory general checklist. Northeld (IL): College of American Pathologists; 2006. [9] Silva MA, editor. Standards for blood banks and transfusion services. 24th edition. Bethesda (MD): AABB; 2006. [10] CLSI [Formerly NCCLS]. CLSI/NCCLS document GP5d Clinical laboratory waste management; approved guideline. 2nd edition. Wayne (PA): Clinical and Laboratory Standards Institute; 2002. [11] CLSI [Formerly NCCLS]. CLSI/NCCLS document M29dProtection of laboratory workers from infectious disease transmitted by blood, body uids, and tissue; approved guideline. 4th edition. Wayne (PA): Clinical and Laboratory Standards Institute; 2003. [12] Centers for Disease Control and Prevention. Public health service guidelines for the management of occupational exposures to HBC, HCV, and HIV, and recommendations for post-exposure prophylaxis. Morb Mortal Wkly Rep 2001;50:152. [13] Radiation safety manual. Urbana-Champaign (IL): University of Illinois, 2006. Available at: http://phantom.ehs.uihc.edu/rss/manuals/radiationmanual/pdf/manual.pdf. Accessed on May 15, 2007.
. [14] Laboratory Accreditation Program. Team leader assessment of director and quality checklist. Northeld, IL: College of American Pathologists; 2006 [16] Q-PROBES. Northeld (IL): College of American Pathologists. Available at: www.cap.org. Accessed May 14, 2007. [17] Q-TRACKS. Northeld (IL): College of American Pathologists. Available at: www.cap.org. Accessed May 14, 2007. [18] Russell JP, editor. The ASQ auditing handbook. 3rd edition. Milwaukee (WI): American Society for Quality Press; 2006. [19] Liker J. The Toyota way: 14 management principles from the worlds greatest manufacturer. New York: McGraw-Hill; 2004. [20] Condel JL, Sharbaugh DT, Raab SS. Error-free pathology: applying lean production methods to anatomic pathology. Clin Lab Med 2004;24(4):86599. [21] McDowell J. Getting the fat out of labs. Clinical Laboratory News 2005;31(3):16. [22] Joseph TP. Design a lean laboratory layout. Med Lab Obs 2006;38(2):2431. [23] Joseph TP. Design of lean work cells: a lean laboratory layout (Part II). Med Lab Obs 2006; 38(8):2432. [24] Zidel TG. A lean guide to transforming healthcare: How to implement lean principles in hospitals, medical oces, clinics, and other healthcare organizations. Milwaukee (WI): American Society for Quality Press; 2007.
[25] Brassard M, Finn L, Ginn D, et al. The Six Sigma Memory Jogger II. Salem (NH): GOALQPC; 2002. [26] Riebking N, Tria L. Six Sigma project reduces analytical errors in an automated lab. Med Lab Obs 2005;37(6):203. [27] Barry R, Murcko AC, Brubaker CE. The Six Sigma book for healthcare. Chicago: Health administration Press; 2002. [28] Nevalainen D, Berte L, Kraft C, et al. Evaluating laboratory performance on quality indicators with the Six Sigma scale. Arch Pathol Lab Med 2000;124:5169. [29] Berte LM. Patient safety: Getting there from here. Clinical Laboratory Management Review 2004;18(6):3115. [30] Daley AT. Pro: Lean Six Sigma revolutionizing health care of tomorrow. Available at: www. clma.org/les/publes/clmr/PDF/Sep-Oct_2006/daley.pdf. Accessed on May 15, 2007. [31] Caldwell C, Brexler J, Gillem T. Lean Six Sigma for healthcare: A senior leader guide to improving cost and throughput. Milwaukee (WI): American Society for Quality Press; 2005. [32] Landek D. Con: Six Sigma is not always the right answer in the clinical laboratory. Available at: www.clma.org/les/publes/clmr/PDF/Sep-Oct_2006/landek.pdf. Accessed on May 15, 2007. [33] Berte LM. Managing laboratory quality: A systematic approach. Lab Med 2004;35(10): 6214. [34] Available at: http://enews.clsi.org/clsi/issues/2007-04-01/3.html. Accessed on May 15, 2007. [35] Berwout Sarah, Morrisa Michael and Elisabeth Dequeker Approaches to quality management and accreditation in a genetic testing laboratory. European Journal of Human Genetics (2010) 18, S1S19 & 2010 [36] Kubler-Ross E, Kessler D: On grief and grieving: nding the meaning of grief through the ve stages of loss, 2005. Available at: http://grief.com/the-five-stages-of-grief/ [37] Available at: http://psmile.org/home.cfm [38] Available at: http://wwwn.cdc.gov/mlp/qiconference/Presentations/ZARBO-CDC.pdf
The Twelve Quality System Essentials in Laboratory Certification and Accreditations:
You might also like
- Standard Lab SOPDocument6 pagesStandard Lab SOPrm101520271No ratings yet
- Guidelines For Validation of Analytical ProceduresDocument17 pagesGuidelines For Validation of Analytical ProceduresnickoRiesNo ratings yet
- Guide to Pharmaceutical Quality Control Lab InspectionsDocument16 pagesGuide to Pharmaceutical Quality Control Lab Inspectionssubrata1No ratings yet
- Floor Plan of LaboratoryDocument5 pagesFloor Plan of LaboratoryNorhida PantaranNo ratings yet
- ICSH Guidelines For The Evaluation of Blood Cell AnalysersDocument16 pagesICSH Guidelines For The Evaluation of Blood Cell Analyserssellappan marappanNo ratings yet
- Validate Qualitative Test Method ResultsDocument2 pagesValidate Qualitative Test Method ResultsShaheer BadarNo ratings yet
- Validation of HPLC Techniques For Pharmaceutical AnalysisDocument54 pagesValidation of HPLC Techniques For Pharmaceutical Analysisfatos-osmani-5248No ratings yet
- HPLC Method Devolopment and Validation For EverolimusDocument20 pagesHPLC Method Devolopment and Validation For EverolimusthesisNo ratings yet
- 4.1a.improvisation of Science ApparatusDocument9 pages4.1a.improvisation of Science Apparatusjane-661970% (10)
- ISO verification requirementsDocument3 pagesISO verification requirementsPets Villand100% (1)
- Microbiology Best Laboratory PracticesDocument47 pagesMicrobiology Best Laboratory PracticesQAV_CRS100% (1)
- ICH Quality Guidelines: An Implementation GuideFrom EverandICH Quality Guidelines: An Implementation GuideAndrew TeasdaleNo ratings yet
- Final 1 - Hairul - SS 641 Standards Adoption Workshop - 27 Jun 2019 - Chapter 4 5Document24 pagesFinal 1 - Hairul - SS 641 Standards Adoption Workshop - 27 Jun 2019 - Chapter 4 5Gan Yi ZheNo ratings yet
- Guidelines For Safe Work Practices in Human and Animal Clinical Diagnostic LaboratoriesDocument352 pagesGuidelines For Safe Work Practices in Human and Animal Clinical Diagnostic LaboratoriesAndreasNo ratings yet
- Chpt13 Quality Control AssuranceDocument7 pagesChpt13 Quality Control Assurancevisini100% (1)
- Validacio Microbio.Document15 pagesValidacio Microbio.cgannauNo ratings yet
- Alternative Micro Methods in Pharma: Need for New Micro CurriculumDocument9 pagesAlternative Micro Methods in Pharma: Need for New Micro Curriculumltrevino100No ratings yet
- Internal Quality Control Practices in Coagulation LaboratoriesDocument10 pagesInternal Quality Control Practices in Coagulation LaboratoriesMy LeNo ratings yet
- Guide To AutoclavingDocument12 pagesGuide To AutoclavingAndrew TurnerNo ratings yet
- Aseptic Processing Case StudyDocument28 pagesAseptic Processing Case Studykavya nainitaNo ratings yet
- IVT Sterility Test Failure InvestigationsDocument8 pagesIVT Sterility Test Failure InvestigationsVinoth KumarNo ratings yet
- Clia & Cap Regulatory TrainingDocument23 pagesClia & Cap Regulatory TrainingWilliam David HommelNo ratings yet
- The APIC Audit ProgrammeDocument19 pagesThe APIC Audit ProgrammeshdphNo ratings yet
- Laboratory ManagementDocument1 pageLaboratory ManagementAj NazarioNo ratings yet
- AACB 2013 Lab QCDocument9 pagesAACB 2013 Lab QCMW100% (1)
- Microbiology Quality ControlDocument31 pagesMicrobiology Quality ControlZeeshan YousufNo ratings yet
- Science Lab RulesDocument6 pagesScience Lab RulesMalati PalanisamyNo ratings yet
- Leaning The Quality Control LaboratoryDocument7 pagesLeaning The Quality Control LaboratoryNarongchai PongpanNo ratings yet
- Good Laboratory PracticeDocument12 pagesGood Laboratory PracticeVllsS100% (1)
- 2019 Phlebotomy Student HandbookDocument47 pages2019 Phlebotomy Student HandbookMohamed NourNo ratings yet
- Microbiological Documentation: Non-Conformances by Tim SandleDocument21 pagesMicrobiological Documentation: Non-Conformances by Tim SandleTim Sandle100% (2)
- Quality Process and Control in Cell ProductionDocument22 pagesQuality Process and Control in Cell ProductionCaths AprilliaNo ratings yet
- Qualityassuranceinmedicallaboratory 190816140948Document75 pagesQualityassuranceinmedicallaboratory 190816140948SEHELY AFSANANo ratings yet
- GP33 Manual ClsiDocument3 pagesGP33 Manual ClsiGonzalez ArturoNo ratings yet
- PPTDocument48 pagesPPTMukesh KumarNo ratings yet
- SopDocument11 pagesSopkssehrawat100% (1)
- IVT Network - Sanitization of Pharmaceutical Facilities - 2014-08-29Document7 pagesIVT Network - Sanitization of Pharmaceutical Facilities - 2014-08-29Bhagath VikasNo ratings yet
- 4.1-5 Training PlanDocument15 pages4.1-5 Training PlanChiropractic Marketing NowNo ratings yet
- Basic Clinical Lab ManagemenDocument38 pagesBasic Clinical Lab ManagemenanggieNo ratings yet
- FDA CGMP Laboratory Controls GuidanceDocument51 pagesFDA CGMP Laboratory Controls GuidanceTarikNo ratings yet
- An Inside Look at USP71Document22 pagesAn Inside Look at USP71Dante IulliNo ratings yet
- A Final Floor Show For Bugs (Sandle)Document4 pagesA Final Floor Show For Bugs (Sandle)Tim Sandle100% (1)
- 0108 - Change Managament Enabling Quality - Doyle - P10 - FINALDocument14 pages0108 - Change Managament Enabling Quality - Doyle - P10 - FINALCesar Rodolfo Angulo DelgadoNo ratings yet
- Clinical Chemistry - SamplesDocument105 pagesClinical Chemistry - SamplesSamar SharafNo ratings yet
- Iso 15189Document15 pagesIso 15189Rai MelindaNo ratings yet
- 04.01 LQTS Free Lime Analysis by Complexometry Method - ENGDocument12 pages04.01 LQTS Free Lime Analysis by Complexometry Method - ENGrupesh soniNo ratings yet
- Quality in The Clinical Microbiology LaboratoryDocument43 pagesQuality in The Clinical Microbiology LaboratoryYemen IlimaneNo ratings yet
- Microbiology Product Catalog EU enDocument94 pagesMicrobiology Product Catalog EU enArifin R HidayatNo ratings yet
- Point of Care Testing Policy Guideline: Edition 1: 2016Document40 pagesPoint of Care Testing Policy Guideline: Edition 1: 2016Paul100% (1)
- Orientation To Clinical Biochemistry-PreanalyticalDocument6 pagesOrientation To Clinical Biochemistry-PreanalyticalasjxhiBBniu01j2No ratings yet
- How To Successfully Implement A DisinfectantDocument2 pagesHow To Successfully Implement A DisinfectantTim Sandle100% (1)
- Responding To Regulatory InspectionsDocument5 pagesResponding To Regulatory Inspectionspradeep281001No ratings yet
- Environmental Monitoring Incubation Conditions - JustificationDocument4 pagesEnvironmental Monitoring Incubation Conditions - Justificationveerreddy_157808No ratings yet
- Guidelines For Cell LinesDocument26 pagesGuidelines For Cell LinesexecNo ratings yet
- Quality Control of Culture Media in A Microbiology LaboratoryDocument6 pagesQuality Control of Culture Media in A Microbiology LaboratoryAtolye GepettoNo ratings yet
- QBD EMEA PPTDocument21 pagesQBD EMEA PPTElizabethValverde100% (1)
- PHSS Annual Members Conference 2014: Book Online Phss - Co.uk/eventsDocument3 pagesPHSS Annual Members Conference 2014: Book Online Phss - Co.uk/eventsTim SandleNo ratings yet
- Cleaning Reverse Phase ColumnDocument2 pagesCleaning Reverse Phase ColumnhbordasmNo ratings yet
- Cumitech 39Document18 pagesCumitech 39nydiacastillom2268100% (1)
- AMP AssayValidation FinalDocument12 pagesAMP AssayValidation FinalMario Salinas100% (1)
- Laboratory Biorisk Management CWA 15793Document46 pagesLaboratory Biorisk Management CWA 15793LESP COLIMA50% (2)
- Validation of Viral Clearance: S K Patel College of Pharmaceutical Education & Research Ganpat UniversityDocument24 pagesValidation of Viral Clearance: S K Patel College of Pharmaceutical Education & Research Ganpat UniversitynirmalpharmaNo ratings yet
- Point-of-Care Testing EssentialsDocument40 pagesPoint-of-Care Testing EssentialsPrincewill Seiyefa100% (1)
- SOP of Gram StainDocument5 pagesSOP of Gram Stainzalam55100% (1)
- CLIA Report Response and ActionsDocument172 pagesCLIA Report Response and ActionsThe Salt Lake TribuneNo ratings yet
- Method Evaluation (Validation) and Method Comparison: - The Analytical Quality Triangle - Purpose of Method EvaluationDocument11 pagesMethod Evaluation (Validation) and Method Comparison: - The Analytical Quality Triangle - Purpose of Method Evaluationoula78No ratings yet
- Data Integrity and Compliance: A Primer for Medical Product ManufacturersFrom EverandData Integrity and Compliance: A Primer for Medical Product ManufacturersNo ratings yet
- Molecular Biological Markers for Toxicology and Risk AssessmentFrom EverandMolecular Biological Markers for Toxicology and Risk AssessmentNo ratings yet
- dm2021-0332 Guidelines For The Implementation of QAP of COVID 19 LaboratoriesDocument16 pagesdm2021-0332 Guidelines For The Implementation of QAP of COVID 19 LaboratoriesJoselito P. PlatillaNo ratings yet
- Lists of Nba FilesDocument2 pagesLists of Nba FilesCIPET IQAC100% (1)
- Health, Safety and Environmental Policies and Procedures ManualDocument64 pagesHealth, Safety and Environmental Policies and Procedures ManualBenaoumeur FertasNo ratings yet
- BMG Labtech Thermostar Manual EngDocument10 pagesBMG Labtech Thermostar Manual EngShan AhmadNo ratings yet
- HBRC ملخصoDocument77 pagesHBRC ملخصoalaa_hassan999_37034No ratings yet
- Brochure FinalDocument2 pagesBrochure FinalnatarajaNo ratings yet
- Grace Hageman - ResumeDocument1 pageGrace Hageman - Resumeapi-531647545No ratings yet
- Laboratory Management Lesson 1: Introduction To Management: A. Cause-And-Effect AnalysisDocument34 pagesLaboratory Management Lesson 1: Introduction To Management: A. Cause-And-Effect AnalysisAngelica Camille B. AbaoNo ratings yet
- Hemax530AL Service Manual PDFDocument175 pagesHemax530AL Service Manual PDFÂn Đình100% (1)
- Family Health Nursing Process (Final)Document89 pagesFamily Health Nursing Process (Final)Arella FloresNo ratings yet
- Laboratory Safety and GlasswareDocument7 pagesLaboratory Safety and Glasswareفهد سعيد ال مطره الغامديNo ratings yet
- Safety Contract From FlinnDocument1 pageSafety Contract From Flinnapi-219812589No ratings yet
- Hazardous Waste Disposal Policy / Procedure in The Chemical Hygiene GuideDocument3 pagesHazardous Waste Disposal Policy / Procedure in The Chemical Hygiene GuideJoko LastyonoNo ratings yet
- Flinn Safety FormDocument1 pageFlinn Safety Formapi-295147740No ratings yet
- Syllabus Applied PhysicsDocument2 pagesSyllabus Applied PhysicsLidya FasilNo ratings yet
- HOKLAS - SC-20 Procedure For Validation MethodDocument17 pagesHOKLAS - SC-20 Procedure For Validation MethodAgeng Wahyu PatrianitaNo ratings yet
- Education and Productivity in NigeriaDocument21 pagesEducation and Productivity in NigeriaJennifer Garuba100% (1)
- OOSDocument14 pagesOOSqfbfabyholaNo ratings yet
- CCLec P1 - Laboratory Safety and Patient PreparationDocument6 pagesCCLec P1 - Laboratory Safety and Patient PreparationRyle PanesNo ratings yet
- Postdoctoral Position in The Physics of Porous Materials and Energy ApplicationsDocument3 pagesPostdoctoral Position in The Physics of Porous Materials and Energy ApplicationsChristos StiapisNo ratings yet
- Lab Manual For Production Technology: January 2020Document68 pagesLab Manual For Production Technology: January 2020MEWAEL MIZANNo ratings yet
- Loreto National High School TLE Daily Lesson Log for Maintaining Computer and Network SystemsDocument4 pagesLoreto National High School TLE Daily Lesson Log for Maintaining Computer and Network SystemsMary GraceNo ratings yet