You might also like
- IDCAP Fact SheetDocument2 pagesIDCAP Fact SheetIDCAP2011No ratings yet
- IDCAP Fact SheetDocument2 pagesIDCAP Fact SheetIDCAP2011No ratings yet
- ASTMH HMIS UgandaDocument1 pageASTMH HMIS UgandaIDCAP2011No ratings yet
- Innovation in Impact EvaluationDocument13 pagesInnovation in Impact EvaluationIDCAP2011No ratings yet
- Computerized Health Facility Outpatient Visit FormDocument1 pageComputerized Health Facility Outpatient Visit FormIDCAP2011No ratings yet
- 54th ECSA Health Ministers' Conference Mombasa, KenyaDocument29 pages54th ECSA Health Ministers' Conference Mombasa, KenyaIDCAP2011No ratings yet
- On-Site Support Participation by Rural Mid-Level Health Practitioners in UgandaDocument1 pageOn-Site Support Participation by Rural Mid-Level Health Practitioners in UgandaIDCAP2011No ratings yet
- IDCAPDocument1 pageIDCAPIDCAP2011No ratings yet
- Impact of OSS On Malaria Management 2011Document1 pageImpact of OSS On Malaria Management 2011IDCAP2011No ratings yet
- Improving Outpatient Health Management Systems in UgandaDocument1 pageImproving Outpatient Health Management Systems in UgandaIDCAP2011No ratings yet
- Mid-Level Practitioners' Role in Managing Infectious Diseases and Site LeadershipDocument10 pagesMid-Level Practitioners' Role in Managing Infectious Diseases and Site LeadershipIDCAP2011No ratings yet
- Improving Human Resources Capacity Through Evidence-Based TrainingDocument14 pagesImproving Human Resources Capacity Through Evidence-Based TrainingIDCAP2011No ratings yet
- Advances in Medical EducationDocument1 pageAdvances in Medical EducationIDCAP2011No ratings yet
- Case Scenario Final Presentation Montreal GHC 2011Document8 pagesCase Scenario Final Presentation Montreal GHC 2011IDCAP2011No ratings yet
- IDCAP Bibliography (As of November 1, 2011) : Lancet. 2009 374 (9687) : 393-403Document10 pagesIDCAP Bibliography (As of November 1, 2011) : Lancet. 2009 374 (9687) : 393-403IDCAP2011No ratings yet
- IDCAP Bibliography (As of November 1, 2011) : Lancet. 2009 374 (9687) : 393-403Document10 pagesIDCAP Bibliography (As of November 1, 2011) : Lancet. 2009 374 (9687) : 393-403IDCAP2011No ratings yet
- IDCAP ResourcesDocument1 pageIDCAP ResourcesIDCAP2011No ratings yet
- IDCAP Clinical Assessment ToolsDocument4 pagesIDCAP Clinical Assessment ToolsIDCAP2011100% (1)
- Sample Case ScenarioDocument6 pagesSample Case ScenarioIDCAP2011No ratings yet
- On-Site SupportDocument2 pagesOn-Site SupportIDCAP2011No ratings yet
- IDCAP Mobile TeamsDocument2 pagesIDCAP Mobile TeamsIDCAP2011No ratings yet
- Integrated Management of Infectious Disease (IMID)Document3 pagesIntegrated Management of Infectious Disease (IMID)IDCAP2011No ratings yet
- IDCAP Data Surveillance SystemDocument5 pagesIDCAP Data Surveillance SystemIDCAP2011No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Letter of Recommendation For Nicolas Hallett From Big Ten Network's Casey Peterson.Document1 pageLetter of Recommendation For Nicolas Hallett From Big Ten Network's Casey Peterson.Nic HallettNo ratings yet
- SIWES Report Example For Civil Engineering StudentDocument46 pagesSIWES Report Example For Civil Engineering Studentolayinkar30No ratings yet
- For-tea Tea Parlour Marketing Strategy Targets 40+ DemographicDocument7 pagesFor-tea Tea Parlour Marketing Strategy Targets 40+ Demographicprynk_cool2702No ratings yet
- Introduction to Human Resource Management Functions and Their ImportanceDocument23 pagesIntroduction to Human Resource Management Functions and Their ImportancedhrupaNo ratings yet
- StrutsDocument7 pagesStrutsBatrisyialya RusliNo ratings yet
- C - Official Coast HandbookDocument15 pagesC - Official Coast HandbookSofia FreundNo ratings yet
- How To Open and Convert An .SCM FileDocument5 pagesHow To Open and Convert An .SCM FilejackNo ratings yet
- Sap Fi/Co: Transaction CodesDocument51 pagesSap Fi/Co: Transaction CodesReddaveni NagarajuNo ratings yet
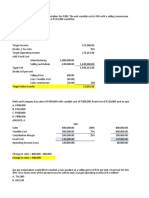
- CVP Solution (Quiz)Document9 pagesCVP Solution (Quiz)Angela Miles DizonNo ratings yet
- Fleck 3150 Downflow: Service ManualDocument40 pagesFleck 3150 Downflow: Service ManualLund2016No ratings yet
- A Dream Takes FlightDocument3 pagesA Dream Takes FlightHafiq AmsyarNo ratings yet
- A - Bahasa Inggris-DikonversiDocument96 pagesA - Bahasa Inggris-DikonversiArie PurnamaNo ratings yet
- Perbandingan Sistem Pemerintahan Dalam Hal Pemilihan Kepala Negara Di Indonesia Dan SingapuraDocument9 pagesPerbandingan Sistem Pemerintahan Dalam Hal Pemilihan Kepala Negara Di Indonesia Dan SingapuraRendy SuryaNo ratings yet
- BUSN7054 Take Home Final Exam S1 2020Document14 pagesBUSN7054 Take Home Final Exam S1 2020Li XiangNo ratings yet
- Ultrasonic Inspection Standards for Wrought MetalsDocument44 pagesUltrasonic Inspection Standards for Wrought Metalsdomsoneng100% (1)
- Wordbank Restaurants 15Document2 pagesWordbank Restaurants 15Obed AvelarNo ratings yet
- MMPX 403 Parametr ListDocument30 pagesMMPX 403 Parametr ListOğuz Kağan ÖkdemNo ratings yet
- (Lesson 10-1) - Quality Assurance, Hemocytometry, Thoma PipetsDocument22 pages(Lesson 10-1) - Quality Assurance, Hemocytometry, Thoma PipetselleNo ratings yet
- Shri Siddheshwar Co-Operative BankDocument11 pagesShri Siddheshwar Co-Operative BankPrabhu Mandewali50% (2)
- Merlin Gerin Medium VoltageDocument10 pagesMerlin Gerin Medium VoltagekjfenNo ratings yet
- The Earthing of Zenner BarrierDocument4 pagesThe Earthing of Zenner BarrierFatholla SalehiNo ratings yet
- Rejoinder To Adom Ochere's Misrepresentation - FinalDocument3 pagesRejoinder To Adom Ochere's Misrepresentation - FinalFuaad DodooNo ratings yet
- ABN AMRO Holding N.V. 2009 Annual ReportDocument243 pagesABN AMRO Holding N.V. 2009 Annual ReportF.N. HeinsiusNo ratings yet
- 3000W InverterDocument2 pages3000W InverterSeda Armand AllaNo ratings yet
- Modulus of Subgrade Reaction KsDocument1 pageModulus of Subgrade Reaction KsmohamedabdelalNo ratings yet
- Exam Venue For Monday Sep 25, 2023 - 12-00 To 01-00Document7 pagesExam Venue For Monday Sep 25, 2023 - 12-00 To 01-00naveed hassanNo ratings yet
- Library Management System (Final)Document88 pagesLibrary Management System (Final)Ariunbat Togtohjargal90% (30)
- The Non Technical Part: Sample Interview Questions For Network EngineersDocument5 pagesThe Non Technical Part: Sample Interview Questions For Network EngineersblablaNo ratings yet
- Localization Strategy in Vietnamese Market: The Cases ofDocument25 pagesLocalization Strategy in Vietnamese Market: The Cases ofHồng Thy NguyễnNo ratings yet
- Sample Contract Rates MerchantDocument2 pagesSample Contract Rates MerchantAlan BimantaraNo ratings yet