You might also like
- 33333determination of Water - and Fat-Soluble Vitamins in D555i ErentDocument21 pages33333determination of Water - and Fat-Soluble Vitamins in D555i ErentmohammaddammagNo ratings yet
- DMF Guidance For Submission V 1.0Document14 pagesDMF Guidance For Submission V 1.0Raj DesaiNo ratings yet
- Impact of Employee's Behavior and Culture On OrganizationsDocument3 pagesImpact of Employee's Behavior and Culture On Organizationseclipse541No ratings yet
- Overview:: Environmental Risks & ImpactDocument28 pagesOverview:: Environmental Risks & ImpactGoffiNo ratings yet
- 26252.9.6. Uniformity of Content of Single-Dose PreparationsDocument1 page26252.9.6. Uniformity of Content of Single-Dose PreparationsMiyyada Aichaoui100% (1)
- Comparing COVID 19 Vaccines For Their Characteristics, EfficacyDocument61 pagesComparing COVID 19 Vaccines For Their Characteristics, EfficacyYony GutierrezNo ratings yet
- Variation GuidelineDocument33 pagesVariation GuidelineBo RatchadapornNo ratings yet
- Guideline On Stability Testing For Applications For Variations To A Marketing AuthorisationDocument8 pagesGuideline On Stability Testing For Applications For Variations To A Marketing Authorisation刘朝阳No ratings yet
- What Is 21 CFR Part 11Document26 pagesWhat Is 21 CFR Part 11chemtabNo ratings yet
- USP Verification of Comp en Dial Procedures CVG CADocument23 pagesUSP Verification of Comp en Dial Procedures CVG CAWilliamWang19No ratings yet
- 1-6 Establishing Impurity SpecificationsDocument52 pages1-6 Establishing Impurity SpecificationsDivyesh PatelNo ratings yet
- The Impact of Culture On An OrganizationDocument4 pagesThe Impact of Culture On An OrganizationSivaraman P. S.No ratings yet
- SHIFADocument4 pagesSHIFAAbira Bilal Hanif0% (1)
- Abraham Lincoln: ContactDocument1 pageAbraham Lincoln: ContactMiguel Angel Condori RoqueNo ratings yet
- Mettler DL36 Operating InstructionsDocument44 pagesMettler DL36 Operating InstructionsLadycorinth137No ratings yet
- P07 CALA ApplicationDocument26 pagesP07 CALA ApplicationCDOKEP2010No ratings yet
- Clean Air and Containment Review: Issue 26 April 2016Document19 pagesClean Air and Containment Review: Issue 26 April 2016Ayman EshraNo ratings yet
- 4 Egac SystemDocument55 pages4 Egac SystemWaleed El-azabNo ratings yet
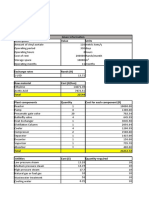
- Group 08 Financial Feasibility Excel 2Document8 pagesGroup 08 Financial Feasibility Excel 2Slindokuhle ThandoNo ratings yet
- 25 How To Determine The Total Impurities - Which Peaks Can Be DisregardedDocument5 pages25 How To Determine The Total Impurities - Which Peaks Can Be Disregardedjljimenez1969100% (1)
- Variations TGADocument128 pagesVariations TGAJaime Andrés García BNo ratings yet
- How To Ensure Trouble-Free HPLC System OperationDocument3 pagesHow To Ensure Trouble-Free HPLC System OperationKavisa GhoshNo ratings yet
- Care Maintenance and HPLC Column TroubleshootingDocument52 pagesCare Maintenance and HPLC Column TroubleshootingJuan R MartinezNo ratings yet
- Suppositories SampleDocument20 pagesSuppositories SamplePriyanka S. SutarNo ratings yet
- Chapter #3 Attitudes and Job SatisfactionDocument2 pagesChapter #3 Attitudes and Job SatisfactionMuhammad Hashim MemonNo ratings yet
- Sample Working Capital Per Dollar of Sales Calculation: Total Sales Income StatementDocument7 pagesSample Working Capital Per Dollar of Sales Calculation: Total Sales Income StatementsanjusarkarNo ratings yet
- Guidelines For Stability Testing of New Drug Substances and ProductsDocument44 pagesGuidelines For Stability Testing of New Drug Substances and Productsvijayns_250355172No ratings yet
- Gas Chromatography - 2 OVIDocument32 pagesGas Chromatography - 2 OVIyashpandya01No ratings yet
- Chromatography IVDocument55 pagesChromatography IVRussell ChuaNo ratings yet
- Missing Functional Level Access Control: OWASP Web App Top 10Document6 pagesMissing Functional Level Access Control: OWASP Web App Top 10erickNo ratings yet
- Simultaneous Determination of Methylparaben + Propylparaben + Hidrocortisone Topical Cream PDFDocument7 pagesSimultaneous Determination of Methylparaben + Propylparaben + Hidrocortisone Topical Cream PDFNájla KassabNo ratings yet
- Omgoing Stability Testing - Innovations - in - Pharmaceutical - TechnologyDocument3 pagesOmgoing Stability Testing - Innovations - in - Pharmaceutical - TechnologyJuan RojasNo ratings yet
- Softening Time Determination of Lipophilic Suppositories: The International Pharmacopoeia - Ninth Edition, 2019Document2 pagesSoftening Time Determination of Lipophilic Suppositories: The International Pharmacopoeia - Ninth Edition, 2019kudzai ashleyNo ratings yet
- Ich - Guideline For Residual SolventsDocument29 pagesIch - Guideline For Residual Solventscssato5No ratings yet
- Verification of System Suitability TestDocument6 pagesVerification of System Suitability TestMubarak PatelNo ratings yet
- OQ Raw Materials Sample TentDocument18 pagesOQ Raw Materials Sample TentAnup BajracharyaNo ratings yet
- Attachment 13 Analytical Equipment Calibration Certificate v3 PDFDocument40 pagesAttachment 13 Analytical Equipment Calibration Certificate v3 PDFGnanaSunderNo ratings yet
- Ion Pairing Reagents and BuffersDocument6 pagesIon Pairing Reagents and BuffersipatoffNo ratings yet
- Quality Control in Aseptic DispensingDocument61 pagesQuality Control in Aseptic DispensingAwal D'LiraNo ratings yet
- Comparison of The EC-GMP Guide Part I With The SFDA-GMP Guideline For Chinese CompaniesDocument7 pagesComparison of The EC-GMP Guide Part I With The SFDA-GMP Guideline For Chinese Companiesrambabukomati472No ratings yet
- Ich Guideline q7 Good Manufacturing Practice Active Pharmaceutical Ingredients Questions Answers - enDocument37 pagesIch Guideline q7 Good Manufacturing Practice Active Pharmaceutical Ingredients Questions Answers - ensatishNo ratings yet
- Canadian-GMPs For DrugsDocument100 pagesCanadian-GMPs For DrugsAnil Kumar GuptaNo ratings yet
- Uniformity Dosage Unit USPDocument4 pagesUniformity Dosage Unit USPwike marelitaNo ratings yet
- Periodic or Skip Testing in Pharmaceutical Industry Us and Europe Perspective 2153 2435.1000283 PDFDocument5 pagesPeriodic or Skip Testing in Pharmaceutical Industry Us and Europe Perspective 2153 2435.1000283 PDFnsk79in@gmail.comNo ratings yet
- WHOPIR LPR 04-06dec2019Document13 pagesWHOPIR LPR 04-06dec20196E.57Pawar RushiNo ratings yet
- Global CRO Scenario & Marketing StrategyDocument21 pagesGlobal CRO Scenario & Marketing StrategyArun Singh SikarwarNo ratings yet
- Guideline On Active Substance Master File Procedure - EuropeanDocument22 pagesGuideline On Active Substance Master File Procedure - EuropeanNhonPhanThanhNo ratings yet
- Internal Customer Satisfaction, Project Report Customer Satisfaction Survey ReportDocument8 pagesInternal Customer Satisfaction, Project Report Customer Satisfaction Survey ReportAnkit MalaniNo ratings yet
- Sodium Lauryl Sulphate BPDocument3 pagesSodium Lauryl Sulphate BPJay PanchaniNo ratings yet
- Satisfaction and Dissatisfaction of JobDocument8 pagesSatisfaction and Dissatisfaction of Jobhanif khanNo ratings yet
- Periodic or Skip Testing in Pharmaceutical Industry Us and Europe Perspective 2153 2435.1000283 PDFDocument5 pagesPeriodic or Skip Testing in Pharmaceutical Industry Us and Europe Perspective 2153 2435.1000283 PDFpakdomoNo ratings yet
- Air Handling Systm in Pharmaceutical Manufacturing Pharm R.A. BinitieDocument86 pagesAir Handling Systm in Pharmaceutical Manufacturing Pharm R.A. BinitieApata olutolaNo ratings yet
- Care of HPLC ColumnsDocument4 pagesCare of HPLC ColumnsKavisa GhoshNo ratings yet
- Data Integrity and Compliance: A Primer for Medical Product ManufacturersFrom EverandData Integrity and Compliance: A Primer for Medical Product ManufacturersNo ratings yet
- Finished Prod 1Document11 pagesFinished Prod 1Ashok KumarNo ratings yet
- Q7 Starting Material Questions and AnswersDocument123 pagesQ7 Starting Material Questions and AnswersDeepak KabburNo ratings yet
- Who Hold Time Studies Rev1 CommentDocument4 pagesWho Hold Time Studies Rev1 CommentschumonNo ratings yet
- HPLC ForumDocument12 pagesHPLC ForumkiranfoodNo ratings yet
- Current Good Manufacturing Practice & Drug Manufacturing QualityDocument54 pagesCurrent Good Manufacturing Practice & Drug Manufacturing QualityGopinath GopiNo ratings yet
- EMA GMP Guidelines For FPDocument13 pagesEMA GMP Guidelines For FPk.p.No ratings yet
- Competitive Assessment and Market Entry Study of Devil's Claw in The USADocument90 pagesCompetitive Assessment and Market Entry Study of Devil's Claw in The USAAnonymous 5i7xlopj8No ratings yet
- Taxofit® Joints Plus Chrono Depot - KlosterfrauDocument2 pagesTaxofit® Joints Plus Chrono Depot - KlosterfrauDušan JovanovićNo ratings yet
- Pharma AtrotoneDocument1 pagePharma AtrotoneKnt Nallasamy GounderNo ratings yet
- LABELSDocument9 pagesLABELSAnton suhendraNo ratings yet
- 209th Meeting (R-II North)Document110 pages209th Meeting (R-II North)Sarfarazpk10% (1)
- GRAS Notice 000666 Chondroitin Sodium SulfateDocument72 pagesGRAS Notice 000666 Chondroitin Sodium SulfateBK RegulatoryNo ratings yet
- TRAT ARTROZA M.fullDocument9 pagesTRAT ARTROZA M.fullSimina BarbuNo ratings yet
- Glucosami̇ne and Chondroi̇ti̇n SulfateDocument4 pagesGlucosami̇ne and Chondroi̇ti̇n Sulfatetaner_soysurenNo ratings yet
- Management of OADocument15 pagesManagement of OARudy HsNo ratings yet
- Condroitina Uebelhart Clinical Review of Chondroitin Sulfate in Osteoarthritis 2008Document3 pagesCondroitina Uebelhart Clinical Review of Chondroitin Sulfate in Osteoarthritis 2008Elisabeth PradoNo ratings yet
- Glucosamine Analysis PDFDocument8 pagesGlucosamine Analysis PDFRidwan OorNo ratings yet
- ESCEO Algoritmo Manejo OADocument9 pagesESCEO Algoritmo Manejo OAMarco LenzNo ratings yet
- Petito Et. Al. v. Piping Rock Health ProductsDocument13 pagesPetito Et. Al. v. Piping Rock Health ProductsPriorSmartNo ratings yet
- Supplements PDFDocument74 pagesSupplements PDFjoey100% (1)
- The Use of Dietary Supplements by AthletesDocument18 pagesThe Use of Dietary Supplements by AthletesSamMKSNo ratings yet
- OsteoarthritisDocument37 pagesOsteoarthritisChikezie Onwukwe100% (1)
- Osteoarthritis ExplanationDocument6 pagesOsteoarthritis ExplanationmedicembuNo ratings yet
- Epigenetic Labs Bone Broth Cookbook 2016Document78 pagesEpigenetic Labs Bone Broth Cookbook 2016Maro T50% (2)
- A Modified Uronic Acid Carbazole Reaction Bitter and Muir 1962Document5 pagesA Modified Uronic Acid Carbazole Reaction Bitter and Muir 1962Levon AntonyanNo ratings yet
- Formularium ApotekDocument12 pagesFormularium ApotekNurul Evi kurniatiNo ratings yet
- Review of Dietary Supplements For The Management of Osteoarthritis in Dogs in Studies From 2004 To 2014Document15 pagesReview of Dietary Supplements For The Management of Osteoarthritis in Dogs in Studies From 2004 To 2014William ChandlerNo ratings yet
- BeeswaxDocument4 pagesBeeswaxLutvi FebriNo ratings yet
- Oral Chondroprotective Agents - Part IDocument7 pagesOral Chondroprotective Agents - Part Itaner_soysurenNo ratings yet
- Chondroitin Sulfate Sodium: Analytical MethodsDocument3 pagesChondroitin Sulfate Sodium: Analytical MethodsAchmad LatiefNo ratings yet
- GlycosaminoglycansDocument31 pagesGlycosaminoglycansAmal100% (1)
- Drug GuidelinesDocument203 pagesDrug GuidelinesPreth Pal SinghNo ratings yet
- OTC wv1Document42 pagesOTC wv1Sheena GagarinNo ratings yet
- Food Supplements Feb2013Document78 pagesFood Supplements Feb2013emmaniago08100% (1)
- Soal STS Genap Bahasa Inggris Kelas 9Document5 pagesSoal STS Genap Bahasa Inggris Kelas 9JAHRAHWATI JAHRAHWATINo ratings yet
- Chronic InflammationDocument28 pagesChronic InflammationFrank NavaNo ratings yet