You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Magnetic Therapy in Eastern Europe A 30 Year ReviewDocument3 pagesMagnetic Therapy in Eastern Europe A 30 Year ReviewMichael McDonnough100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Dien Chan - MultireflexologyDocument136 pagesDien Chan - MultireflexologyDien Chan - Multireflex96% (28)
- Balance Meridean System ChartDocument1 pageBalance Meridean System Chartfuzzface23100% (15)
- Small Animal Neurology Atlas and Textbook-2010 PDFDocument610 pagesSmall Animal Neurology Atlas and Textbook-2010 PDFАнастасия СвириденкоNo ratings yet
- Class 5 Notes - DR Tan's Balancing MethodDocument7 pagesClass 5 Notes - DR Tan's Balancing Methodfuzzface23100% (20)
- Brain Balancing Protocol Dr. Karen March 2014Document5 pagesBrain Balancing Protocol Dr. Karen March 2014Stephen J. RobertsNo ratings yet
- Agnes - Diss VAS NogierDocument114 pagesAgnes - Diss VAS NogierMassiel Socorro Mendez100% (2)
- Needle Less AcupunctureDocument44 pagesNeedle Less AcupunctureOscar Dwn Yap100% (3)
- Oriental Tongue DiagnosisDocument36 pagesOriental Tongue Diagnosissai calder100% (2)
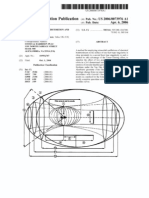
- 10 954 767 Method of Gravity DistortionDocument31 pages10 954 767 Method of Gravity DistortiontogonationNo ratings yet
- Extraction of Timelike Entanglement From The Quantum VacuumDocument8 pagesExtraction of Timelike Entanglement From The Quantum VacuumChad AdamsNo ratings yet
- Neo MiningDocument12 pagesNeo MiningMichael McDonnoughNo ratings yet
- Tuinaology I - TCM 235 NotesDocument6 pagesTuinaology I - TCM 235 NotesRamesh Babu Manivannan100% (1)
- Periodic Test in Health 10Document2 pagesPeriodic Test in Health 10Rialyn EscovillaNo ratings yet
- 2009 Basil Ielts 4 Reading Passage 2Document2 pages2009 Basil Ielts 4 Reading Passage 2elgrecosNo ratings yet
- Medical Apparatus That Can Help Control DiseasesDocument3 pagesMedical Apparatus That Can Help Control DiseasesKrista-Ann KhoNo ratings yet
- McDonald John - Chinese Versus French Perspectives On The Channel SystemDocument17 pagesMcDonald John - Chinese Versus French Perspectives On The Channel SystemAssaf FeldmanNo ratings yet
- Acupuncture Modern MedicineDocument400 pagesAcupuncture Modern MedicineRoberto Biglia100% (5)
- The Miracle of Master Tung's Magic Points:: Correct Tendons' Amazing For Neck PainDocument2 pagesThe Miracle of Master Tung's Magic Points:: Correct Tendons' Amazing For Neck PainMarcin SowNo ratings yet
- Consciousness and Quantum Information PDFDocument14 pagesConsciousness and Quantum Information PDFFaris KulicNo ratings yet
- Alternative System of MedicineDocument13 pagesAlternative System of MedicineDebipriya Mistry100% (1)
- Questions: 1. A. B. C. DDocument33 pagesQuestions: 1. A. B. C. DLavanya SathyaNo ratings yet
- Tips From Chinese Medicine: Self-Care For AnxietyDocument11 pagesTips From Chinese Medicine: Self-Care For Anxietyshamim hijamaNo ratings yet
- Module 20 - Complementary and Alternative MedicineDocument90 pagesModule 20 - Complementary and Alternative Medicinegeekay79No ratings yet
- 23. Đề thi thử TN THPT 2021 - Môn Tiếng anh - THPT Chuyên Trần Phú - Hải Phòng - Lần 1Document9 pages23. Đề thi thử TN THPT 2021 - Môn Tiếng anh - THPT Chuyên Trần Phú - Hải Phòng - Lần 1Linh CottonNo ratings yet
- Acupuncture - Clinical Practice, Particular Techniques and Special Issues 2011Document150 pagesAcupuncture - Clinical Practice, Particular Techniques and Special Issues 2011zzscrib86% (14)
- Health Herald UserDocument17 pagesHealth Herald UserManoel LuizNo ratings yet
- Meridian TherapiesDocument144 pagesMeridian TherapiesJerome Best83% (12)
- Gala Dhiren - Be Your Own Doctor With AcupressureDocument139 pagesGala Dhiren - Be Your Own Doctor With Acupressurebionicras100% (44)
- 5 Element Healing Practitioner Course 2nd ManualDocument99 pages5 Element Healing Practitioner Course 2nd Manualreikiselfmaster86% (7)
- Back Pain by Martin Arrowsmith PDFDocument49 pagesBack Pain by Martin Arrowsmith PDFEd BegsNo ratings yet
- Case Report PresentationDocument19 pagesCase Report PresentationCheyenne PetersNo ratings yet
- Health10 q1 Mod2 Complementary-And-Alternative-Healthcare-Modalities v1Document32 pagesHealth10 q1 Mod2 Complementary-And-Alternative-Healthcare-Modalities v1bayalien nileNo ratings yet
- International College of Traditional Chinese Medicine of VancouverDocument2 pagesInternational College of Traditional Chinese Medicine of Vancouverapi-260294278No ratings yet