You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Worksafe Blood Culture Collection Procedure 1brochDocument1 pageWorksafe Blood Culture Collection Procedure 1brochNidia Maradiaga100% (1)
- Sorloz DiagMicrobiolInfDis51Document3 pagesSorloz DiagMicrobiolInfDis51Nidia MaradiagaNo ratings yet
- Laboratory Based Evaluation of The ColorimetricDocument8 pagesLaboratory Based Evaluation of The ColorimetricNidia MaradiagaNo ratings yet
- Publication HAIDocument56 pagesPublication HAINidia MaradiagaNo ratings yet
- HAI BrochureDocument6 pagesHAI BrochureNidia MaradiagaNo ratings yet
- Etest Brochure 1Document2 pagesEtest Brochure 1Nidia MaradiagaNo ratings yet
- Antibiotic Susceptibility Testing Bacterial Resistance: Questions & Answers OnDocument16 pagesAntibiotic Susceptibility Testing Bacterial Resistance: Questions & Answers OnsazunaxNo ratings yet
- Kus - CMAJ 2011Document5 pagesKus - CMAJ 2011Nidia MaradiagaNo ratings yet
- Antibiotic Susceptibility Testing Bacterial Resistance: Questions & Answers OnDocument16 pagesAntibiotic Susceptibility Testing Bacterial Resistance: Questions & Answers OnsazunaxNo ratings yet
- Poirel - AAC 2010Document4 pagesPoirel - AAC 2010Nidia MaradiagaNo ratings yet
- Pratcical Guide For CDADocument16 pagesPratcical Guide For CDANidia MaradiagaNo ratings yet
- VTK2 AdvancedColorimetryDocument2 pagesVTK2 AdvancedColorimetryNidia MaradiagaNo ratings yet
- Practical Guide For HAI PreventionDocument22 pagesPractical Guide For HAI PreventionNidia MaradiagaNo ratings yet
- VITEK2 CardsDocument4 pagesVITEK2 CardsNidia MaradiagaNo ratings yet
- VTK2 Advanced TechnologyDocument6 pagesVTK2 Advanced TechnologyNidia MaradiagaNo ratings yet
- BTAmediaDocument4 pagesBTAmediaNidia MaradiagaNo ratings yet
- Bac TAlertDocument2 pagesBac TAlertNidia MaradiagaNo ratings yet
- Identifying 6Document6 pagesIdentifying 6Nidia MaradiagaNo ratings yet
- Bac TAlert 60Document2 pagesBac TAlert 60Nidia MaradiagaNo ratings yet
- Identifying 5Document6 pagesIdentifying 5Nidia MaradiagaNo ratings yet
- Expert Systems: Web SitesDocument6 pagesExpert Systems: Web SitesNidia MaradiagaNo ratings yet
- Poster BacT Alert 2 SpanishDocument1 pagePoster BacT Alert 2 SpanishNidia MaradiagaNo ratings yet
- Identifying 7Document6 pagesIdentifying 7Nidia MaradiagaNo ratings yet
- Vitek 2 Compact BrochureDocument2 pagesVitek 2 Compact BrochureNidia MaradiagaNo ratings yet
- Poster BacT Alert 2 SpanishDocument1 pagePoster BacT Alert 2 SpanishNidia MaradiagaNo ratings yet
- EPI Vaccines: - Inactivated (Killed) Microorganisms - Attentuated Microorganisms Fragments From Microorganisms ToxoidsDocument3 pagesEPI Vaccines: - Inactivated (Killed) Microorganisms - Attentuated Microorganisms Fragments From Microorganisms ToxoidsIrene Grace BalcuevaNo ratings yet
- Phenoxymethyl Penicillin Penicillin V Tablet Prescribing InformationDocument2 pagesPhenoxymethyl Penicillin Penicillin V Tablet Prescribing InformationitsshuvroNo ratings yet
- 2.oral Manifestation of Bacterial InfectionDocument18 pages2.oral Manifestation of Bacterial Infectionhesti_margarethaNo ratings yet
- Identification and classification of infections in neonatesDocument62 pagesIdentification and classification of infections in neonatesvisuinsvu100% (7)
- Discovery of ViroidsDocument21 pagesDiscovery of ViroidsKhoo Ying WeiNo ratings yet
- ANTIMICROBIAL SUSCEPTIBILITY TESTING and MYCOBACTERIADocument8 pagesANTIMICROBIAL SUSCEPTIBILITY TESTING and MYCOBACTERIAAlthea Jam Grezshyl GaloNo ratings yet
- TricDocument1 pageTricmadfropNo ratings yet
- Capitulo 8 EnterobacteriaceaeDocument6 pagesCapitulo 8 EnterobacteriaceaeLuis RodriguezNo ratings yet
- ACTIVITY 9 - Biosafety and BiosecurityDocument6 pagesACTIVITY 9 - Biosafety and BiosecurityJaisel Meris Ado-anNo ratings yet
- Expression Ready RFP Retroviral ParticlesDocument1 pageExpression Ready RFP Retroviral ParticlesAlleleBiotechNo ratings yet
- Microscopy Gram-Color: Stain Set For The Gram Staining MethodDocument3 pagesMicroscopy Gram-Color: Stain Set For The Gram Staining MethodMuhammad AdhityaNo ratings yet
- Problem Based Learning: Case StudyDocument27 pagesProblem Based Learning: Case StudyOleOhhNo ratings yet
- Liofilchem: Product Catalogue 2019Document98 pagesLiofilchem: Product Catalogue 2019YuriAlexanderEspinozaPuga100% (1)
- 5-Aseptic BehaviourDocument10 pages5-Aseptic BehaviourMona AlmahdalyNo ratings yet
- Pet MicrobeDocument8 pagesPet MicrobeEmily CribasNo ratings yet
- Gram Positive Bacteria ChartDocument1 pageGram Positive Bacteria ChartPurple basket100% (1)
- Immunization P & SDocument122 pagesImmunization P & SnebilNo ratings yet
- Infectiile Grave Extensive Ale Partilor MoiDocument49 pagesInfectiile Grave Extensive Ale Partilor MoiLoredana BoghezNo ratings yet
- Infection and Infectious Process Power PointDocument44 pagesInfection and Infectious Process Power PointNitesh BhuraNo ratings yet
- Parasitology Lecture NotesDocument8 pagesParasitology Lecture NotesRica DezaNo ratings yet
- Determination of microbiological quality of packed vs unpacked bread and flourDocument7 pagesDetermination of microbiological quality of packed vs unpacked bread and flourHemant OjhaNo ratings yet
- Report On The Antimicrobial Activity of Graminex Nax 7 Paste 1Document13 pagesReport On The Antimicrobial Activity of Graminex Nax 7 Paste 1api-442513573No ratings yet
- Format Pendataan Posyandu Sasaran Bian PKM Pondok Gede JatiwaringinDocument407 pagesFormat Pendataan Posyandu Sasaran Bian PKM Pondok Gede JatiwaringinparamitaNo ratings yet
- MPN Table ExplainedDocument44 pagesMPN Table ExplainedDzulfathil PuteraNo ratings yet
- Medical MicrobiologyDocument62 pagesMedical MicrobiologyJamil Wadud100% (1)
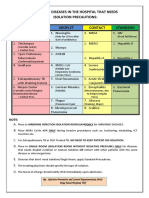
- Common Hospital Diseases Requiring Isolation PrecautionsDocument1 pageCommon Hospital Diseases Requiring Isolation Precautionsjerimiah_manzonNo ratings yet
- Name: - Section: - Schedule: - Class Number: - DateDocument5 pagesName: - Section: - Schedule: - Class Number: - DateAlbieRhioneilLatonioMacayanNo ratings yet
- HFMD: Clinical Features, Complications, Diagnosis and ManagementDocument27 pagesHFMD: Clinical Features, Complications, Diagnosis and ManagementNur IzzahNo ratings yet
- Submerged Culture of The Mycelium of Various Species of MushroomDocument3 pagesSubmerged Culture of The Mycelium of Various Species of Mushroombravohr98No ratings yet
- Microbiology e BookDocument48 pagesMicrobiology e BookWaleed El-azabNo ratings yet