You might also like
- Taat 11 I 3 P 112Document7 pagesTaat 11 I 3 P 112Mike LiebermannNo ratings yet
- Current Trends in Dental ImplantsDocument11 pagesCurrent Trends in Dental ImplantsJavaria IftekharNo ratings yet
- Biomaterials For Dental Implants Current and Future TrendsDocument34 pagesBiomaterials For Dental Implants Current and Future TrendsDeivyson Augusto100% (1)
- Impact of Dental Implant Surface Modifications On OsseointegrationDocument16 pagesImpact of Dental Implant Surface Modifications On OsseointegrationNamrata SNo ratings yet
- 240-Article Text-799-3-10-20190203Document6 pages240-Article Text-799-3-10-20190203EVANDRO FRANCO DA ROCHANo ratings yet
- 240-Article Text-799-3-10-20190203Document6 pages240-Article Text-799-3-10-20190203EVANDRO FRANCO DA ROCHANo ratings yet
- Bone Grafts and Substitutes in DentistryDocument27 pagesBone Grafts and Substitutes in Dentistry林金鋒No ratings yet
- 种植生物材料减少并发症Document13 pages种植生物材料减少并发症xiaoxin zhangNo ratings yet
- 1 s2.0 S0975962X1200024X MainDocument5 pages1 s2.0 S0975962X1200024X MainMr-Ton DrgNo ratings yet
- O.surgery Lec11Document22 pagesO.surgery Lec11MohammedNo ratings yet
- 2006 Implant SurfacesDocument16 pages2006 Implant SurfacesLukas Lopez RamirezNo ratings yet
- Biological Sealing and Defense Mechanisms in Peri-Implant Mucosa of Dental ImplantsDocument25 pagesBiological Sealing and Defense Mechanisms in Peri-Implant Mucosa of Dental ImplantsMar YNo ratings yet
- Immediate Dental Implants and Bone Graft MaterialsDocument11 pagesImmediate Dental Implants and Bone Graft MaterialsAndria FadliNo ratings yet
- Tripplett 2003 - Implant Materials and DesignsDocument18 pagesTripplett 2003 - Implant Materials and DesignsZhiyi LinNo ratings yet
- Fundamentals and History of Implant Dentistry: Tamal Kanti PalDocument8 pagesFundamentals and History of Implant Dentistry: Tamal Kanti PalMaria Beatriz Solis ValenciaNo ratings yet
- Andani 2014Document49 pagesAndani 2014qwerty fkvorkcjdkNo ratings yet
- A Brief Chronological Review of Dental Implant HistoryDocument4 pagesA Brief Chronological Review of Dental Implant HistoryJorge SaenzNo ratings yet
- Latest Bio Materials in Dentistry - Nanaorobots in OrthoDocument22 pagesLatest Bio Materials in Dentistry - Nanaorobots in OrthosivakumarNo ratings yet
- Bone and Metal An Orthopaedic Perspective On Osseointegration of MetalsDocument15 pagesBone and Metal An Orthopaedic Perspective On Osseointegration of MetalsClaudia UngureanuNo ratings yet
- VelmuruganDocument7 pagesVelmuruganMary SmileNo ratings yet
- Ossseointegration of Impl.Document11 pagesOssseointegration of Impl.Claudiu CampeanNo ratings yet
- Accepted Manuscript: Acta BiomaterialiaDocument41 pagesAccepted Manuscript: Acta BiomaterialiaWeihao CaiNo ratings yet
- Current Concepts in Dental ImplantologyDocument274 pagesCurrent Concepts in Dental ImplantologyClaudiu LefterNo ratings yet
- SubstituentiDocument11 pagesSubstituentiBianca Ionela DraganNo ratings yet
- Periodontio Integrated Implants (Ligaplant)Document9 pagesPeriodontio Integrated Implants (Ligaplant)Dr. Minkle GulatiNo ratings yet
- Short Dental Implants Literature ReviewDocument8 pagesShort Dental Implants Literature Reviewttdqgsbnd100% (1)
- Research Paper On Dental ImplantsDocument6 pagesResearch Paper On Dental Implantsafnhekkghifrbm100% (1)
- Review Article: Tooth-Implant Connection: A ReviewDocument8 pagesReview Article: Tooth-Implant Connection: A ReviewDrShweta SainiNo ratings yet
- Gabric D. Dental Implantology Current Concepts. From Science To Clinical... 2022Document355 pagesGabric D. Dental Implantology Current Concepts. From Science To Clinical... 2022Ahmed Abou FoulNo ratings yet
- Materials 12 00154Document19 pagesMaterials 12 00154Marco TeixeiraNo ratings yet
- Orthodontics in 3 Millennia. Chapter 15: Skeletal Anchorage: Special ArticleDocument4 pagesOrthodontics in 3 Millennia. Chapter 15: Skeletal Anchorage: Special ArticleHARITHA H.PNo ratings yet
- Dental Implants: by DR - Mahmoud Ahmed Elfarmawy Lecture of OMFS Faculty of Dentistry, SU, KantaraDocument34 pagesDental Implants: by DR - Mahmoud Ahmed Elfarmawy Lecture of OMFS Faculty of Dentistry, SU, KantaraMohammed TarekNo ratings yet
- Alveolar Ridge Preservation After Tooth Extraction Using Different Bone Graft Materials and Autologous Platelet ConcentratesDocument15 pagesAlveolar Ridge Preservation After Tooth Extraction Using Different Bone Graft Materials and Autologous Platelet ConcentratesnicolesigoloNo ratings yet
- Direct Restoration of Endodontically Treated Teeth A Brief Sumary of Materials and TechnoquesDocument8 pagesDirect Restoration of Endodontically Treated Teeth A Brief Sumary of Materials and Technoquesmaroun ghalebNo ratings yet
- Retrospective Study: Lateral Ridge Augmentation Using Autogenous Dentin: Tooth-Shell Technique vs. Bone-Shell TechniqueDocument12 pagesRetrospective Study: Lateral Ridge Augmentation Using Autogenous Dentin: Tooth-Shell Technique vs. Bone-Shell TechniqueNarissaporn ChaiprakitNo ratings yet
- New Microsoft Office Word DocumentDocument3 pagesNew Microsoft Office Word DocumentAtulsanapNo ratings yet
- BIOMATERIALS IN DENTAL IMPLANTSDocument33 pagesBIOMATERIALS IN DENTAL IMPLANTSNagappan Chockalingam100% (1)
- Implantology and The Severely Resorbed Edentulous MandibleDocument9 pagesImplantology and The Severely Resorbed Edentulous MandibleAfiz ZullahNo ratings yet
- Biomaterials For Dental Implants: Current and Future Trends: Journal of Materials Science July 2015Document37 pagesBiomaterials For Dental Implants: Current and Future Trends: Journal of Materials Science July 2015Seno FauziNo ratings yet
- Microleakage PDFDocument16 pagesMicroleakage PDFbyyou0% (1)
- Mechanical Aspects of Dental ImplantDocument53 pagesMechanical Aspects of Dental ImplantFreddy BenalcázarNo ratings yet
- Overdenture LDDocument71 pagesOverdenture LDDr. SwathiNo ratings yet
- 10.1007@s11837 019 03687 2Document13 pages10.1007@s11837 019 03687 2Sajid NazirNo ratings yet
- DCNA ImplantsDocument16 pagesDCNA ImplantsDentist Here100% (1)
- 01Document142 pages01Praveena SailenthranNo ratings yet
- Periodontology 2000 - 2019 - Guglielmotti - Research on implants and osseointegrationDocument12 pagesPeriodontology 2000 - 2019 - Guglielmotti - Research on implants and osseointegrationalinagaxiolaariasNo ratings yet
- زراعه 1Document5 pagesزراعه 1haidergamer658No ratings yet
- Alloplastic Bone GraftsDocument62 pagesAlloplastic Bone GraftsMaysaa mahdiNo ratings yet
- Ceramic Dental Implants: A Literature ReviewDocument5 pagesCeramic Dental Implants: A Literature ReviewDeepalakshmi VenkatesanNo ratings yet
- Huwais2016 JOMIArticleDocument11 pagesHuwais2016 JOMIArticleHusnul BasyarNo ratings yet
- Clinical and Radiographic of Marginal Periimplant Tissue Stability After Buccal Defect Regeneration Using Porous Titanium GranuDocument12 pagesClinical and Radiographic of Marginal Periimplant Tissue Stability After Buccal Defect Regeneration Using Porous Titanium GranuDrMohamed AssadawyNo ratings yet
- Kim Regenerative EndodonticsDocument51 pagesKim Regenerative Endodonticsrasagna reddyNo ratings yet
- ImplantologyDocument212 pagesImplantologyGabriela Cocieru Motelica100% (1)
- In Uence of Removable Partial Dentures On Plaque AccumulationDocument8 pagesIn Uence of Removable Partial Dentures On Plaque Accumulationlian liaanNo ratings yet
- The Effectiveness of Osseodensification Drilling PDocument19 pagesThe Effectiveness of Osseodensification Drilling PdentureNo ratings yet
- Implant Surface Characteristics and Their Effect On OsseointegrationDocument9 pagesImplant Surface Characteristics and Their Effect On Osseointegrationsnehal jaiswalNo ratings yet
- Reference and Techniques Used in Alveolar Bone ClassificationDocument5 pagesReference and Techniques Used in Alveolar Bone ClassificationAna Carolina LoyolaNo ratings yet
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- PV Module IonDocument4 pagesPV Module IonrmalewarNo ratings yet
- Chemdur - 52Document3 pagesChemdur - 52ICPL-RWPNo ratings yet
- Nanotechnology v1.0Document43 pagesNanotechnology v1.0Faizan AhmedNo ratings yet
- (Chapter 1) Fluid Mechanics For Mechanical EngineeringDocument38 pages(Chapter 1) Fluid Mechanics For Mechanical EngineeringAnn Razon0% (1)
- Refineria de Cartagena (Reficar) Refinery Expansion - Hydrocarbons TechnologyDocument3 pagesRefineria de Cartagena (Reficar) Refinery Expansion - Hydrocarbons TechnologyGjorgeluisNo ratings yet
- Manufacturing porcelain figures using binder jetting 3D printingDocument8 pagesManufacturing porcelain figures using binder jetting 3D printingcesarNo ratings yet
- Shell Rimula R3 Turbo 15W-40Document2 pagesShell Rimula R3 Turbo 15W-40HUM CIREBON DFLTSNo ratings yet
- Carbonyl CompoundsDocument34 pagesCarbonyl CompoundsprinceNo ratings yet
- General Information CoalDocument144 pagesGeneral Information CoalSaravanan RagupathyNo ratings yet
- Zahid Husain M.Pharm (Pharmaceutics) Faculty of Pharmacy, IU, LucknowDocument24 pagesZahid Husain M.Pharm (Pharmaceutics) Faculty of Pharmacy, IU, LucknowQA Dhq OkaraNo ratings yet
- Brochure - Eu Standard Equipment For Commercial Kitchens v1.0 En-WebDocument4 pagesBrochure - Eu Standard Equipment For Commercial Kitchens v1.0 En-WebalanatoraNo ratings yet
- SurgeryDocument79 pagesSurgeryIshratNo ratings yet
- 04 - Metode ElektrogravimetriDocument19 pages04 - Metode ElektrogravimetriNurul Aulia HusainNo ratings yet
- Astm A500Document2 pagesAstm A500Liquor Liam0% (1)
- Material Report: Compound Data SheetDocument3 pagesMaterial Report: Compound Data SheetRanja SarkarNo ratings yet
- Origins of Rheology: A Brief Look at the Evolution of the Study of Material FlowDocument9 pagesOrigins of Rheology: A Brief Look at the Evolution of the Study of Material FlowAmlan PalNo ratings yet
- ICSE Biology Exam 2021Document7 pagesICSE Biology Exam 2021Sarthac JainNo ratings yet
- Tell sth apart = distinguish between sth: phân biệt giữa 2 thứ gìDocument6 pagesTell sth apart = distinguish between sth: phân biệt giữa 2 thứ gìHiền TrầnNo ratings yet
- SF016 Physics Semester 1 Session 2015/2016 1 hour examDocument4 pagesSF016 Physics Semester 1 Session 2015/2016 1 hour examlynnadzNo ratings yet
- SSIP GR 11 Acids N BasesDocument10 pagesSSIP GR 11 Acids N BasesMangwane Sello100% (1)
- Engineering Failure Analysis: Lucjan Witek, Micha Ł Sikora, Feliks Stachowicz, Tomasz TrzepiecinskiDocument10 pagesEngineering Failure Analysis: Lucjan Witek, Micha Ł Sikora, Feliks Stachowicz, Tomasz TrzepiecinskisobhanNo ratings yet
- EIFS performance standardsDocument40 pagesEIFS performance standardsRyan ClarkeNo ratings yet
- Enzymes Lab ReportDocument8 pagesEnzymes Lab ReportMaizamNo ratings yet
- Callister Ch09Document90 pagesCallister Ch09Nemish KanwarNo ratings yet
- SHELL AND TUBE HEAT EXCHANGER DESIGNDocument60 pagesSHELL AND TUBE HEAT EXCHANGER DESIGNniaaparamita100% (1)
- Ex 2disesl IndexDocument6 pagesEx 2disesl IndexSalman AlshammariNo ratings yet
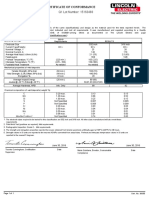
- Certificate of Conformance: Q1 Lot Number: 15163483Document1 pageCertificate of Conformance: Q1 Lot Number: 15163483interx00No ratings yet
- Packaging Materials and Articles For Food: Legislation and Codes of Good Manufacturing PracticeDocument10 pagesPackaging Materials and Articles For Food: Legislation and Codes of Good Manufacturing PracticeMilanVukicNo ratings yet
- Swimming Pool BOQ - Water ProofingDocument2 pagesSwimming Pool BOQ - Water ProofingStephen RajNo ratings yet
- SPE Papers Well DeliverabilityDocument279 pagesSPE Papers Well DeliverabilitySyed Ahmed FlareNo ratings yet