You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 44.0 - Traffic Management and Logistics v3.0 EnglishDocument14 pages44.0 - Traffic Management and Logistics v3.0 EnglishEyob Yimer100% (1)
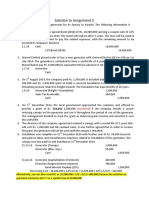
- Assignment 2 SolutionDocument4 pagesAssignment 2 SolutionSobhia Kamal100% (1)
- Format For Computation of Income Under Income Tax ActDocument3 pagesFormat For Computation of Income Under Income Tax ActAakash67% (3)
- Buffet Rule FactsDocument1 pageBuffet Rule Factsben3172No ratings yet
- NY State Fair Tax Petition (First Half)Document29 pagesNY State Fair Tax Petition (First Half)ben3172No ratings yet
- Federal Fair Tax Petition ResultsDocument20 pagesFederal Fair Tax Petition Resultsben3172No ratings yet
- Buffet Editorial 7-14-11Document1 pageBuffet Editorial 7-14-11ben3172No ratings yet
- Occupy CongressDocument1 pageOccupy Congressben3172No ratings yet
- Deregulation Time LineDocument7 pagesDeregulation Time Lineben3172No ratings yet
- Federal Millionaire's Tax Petition TemplateDocument1 pageFederal Millionaire's Tax Petition Templateben3172No ratings yet
- Teachers v. MillionairesDocument1 pageTeachers v. Millionairesben3172No ratings yet
- Minimum Wage PoliticiansDocument1 pageMinimum Wage Politiciansben3172No ratings yet
- Millionaire's Tax Petition TemplateDocument1 pageMillionaire's Tax Petition Templateben3172No ratings yet
- Map of ZuccotiDocument1 pageMap of Zuccotiben3172No ratings yet
- NY State Voter Reg SpanishDocument2 pagesNY State Voter Reg Spanishben3172No ratings yet
- NY State Voter Reg KoreanDocument2 pagesNY State Voter Reg Koreanben3172No ratings yet
- Call Stickers TemplateDocument1 pageCall Stickers Templateben3172No ratings yet
- Occupy Wallstreet FlyerDocument1 pageOccupy Wallstreet Flyerben3172No ratings yet
- Keep The Change PosterDocument1 pageKeep The Change Posterben3172No ratings yet
- The Downstate Update 2011Document9 pagesThe Downstate Update 2011ben3172No ratings yet
- Loadstar Shipping Vs MesanoDocument2 pagesLoadstar Shipping Vs MesanoCuddlyNo ratings yet
- Muzaffarnagar Riots Report - The Jat PerspectiveDocument11 pagesMuzaffarnagar Riots Report - The Jat Perspectivedharma nextNo ratings yet
- 0.US in Caribbean 1776 To 1870Document20 pages0.US in Caribbean 1776 To 1870Tj RobertsNo ratings yet
- Accounting Calling ListDocument4 pagesAccounting Calling Listsatendra singhNo ratings yet
- Elements of Cost SheetDocument11 pagesElements of Cost SheetPratiksha GaikwadNo ratings yet
- GR No. 112497, August 4, 1994 FactsDocument2 pagesGR No. 112497, August 4, 1994 FactsIrene QuimsonNo ratings yet
- Accreditation of NGOs To BBIsDocument26 pagesAccreditation of NGOs To BBIsMelanieParaynoDaban100% (1)
- 26 VANGUARDIA, Cedric F. - COVID Essay PDFDocument1 page26 VANGUARDIA, Cedric F. - COVID Essay PDFEstrell VanguardiaNo ratings yet
- Defensor Santiago v. ComelecDocument15 pagesDefensor Santiago v. ComelecRubierosse DongalloNo ratings yet
- Factorytalk Batch View Quick Start GuideDocument22 pagesFactorytalk Batch View Quick Start GuideNelsonNo ratings yet
- Mana Angel de Amor BassDocument4 pagesMana Angel de Amor BassToreto SantanaNo ratings yet
- 6 Coca-Cola Vs CCBPIDocument5 pages6 Coca-Cola Vs CCBPINunugom SonNo ratings yet
- 2011 Veterans' Hall of Fame Award RecipientsDocument46 pages2011 Veterans' Hall of Fame Award RecipientsNew York SenateNo ratings yet
- Executive Order No. 01-s-2023 (BDC)Document2 pagesExecutive Order No. 01-s-2023 (BDC)kencyrilachasNo ratings yet
- SOP For OLDocument9 pagesSOP For OLTahir Ur RahmanNo ratings yet
- Puss in Boots Esl Printable Reading Comprehension Questions Worksheet For KidsDocument2 pagesPuss in Boots Esl Printable Reading Comprehension Questions Worksheet For KidsauraNo ratings yet
- NaMo Case StudyDocument4 pagesNaMo Case StudyManish ShawNo ratings yet
- ABRAHIM Research .2021.update .Document43 pagesABRAHIM Research .2021.update .Abdi Mucee TubeNo ratings yet
- The History of HRDocument26 pagesThe History of HRsuhasNo ratings yet
- Elc 2009 - Study Pack FullDocument355 pagesElc 2009 - Study Pack FullAllisha BowenNo ratings yet
- Abraham 01Document29 pagesAbraham 01cornchadwickNo ratings yet
- Due Process In India And Fighting Domestic Violence CasesDocument34 pagesDue Process In India And Fighting Domestic Violence CasesSumit Narang0% (1)
- List of Evid CasesDocument3 pagesList of Evid CasesJamie Dilidili-TabiraraNo ratings yet
- Central DirectoryDocument690 pagesCentral DirectoryvmeederNo ratings yet
- BAOLSSDocument3 pagesBAOLSSJahidur RahmanNo ratings yet
- How to Charge Invoices on ERPDocument9 pagesHow to Charge Invoices on ERPClarissa DelgadoNo ratings yet
- Quotation Eoi/Rfp/Rft Process Checklist Goods And/Or ServicesDocument7 pagesQuotation Eoi/Rfp/Rft Process Checklist Goods And/Or ServicesTawanda KurasaNo ratings yet