JOURNAL OF
THE
ROYAL
SOCIETY
OF
MEDICINE
Volume 93
September 2000
Jacobo Mintzer MD
J R Soc Med 2000;93:457462
Alistair Burns MD FRCPsych
Old age is accompanied by an increased likelihood of illness, and old people take a disproportionate amount of selfadministered and prescribed medications. In the USA, people over 65 consume 30% of prescriptions and 40% of over-the-counter remedies, despite making up only 13% of the population1. In the UK, elderly people comprise only 18% of the population but use 45% of all prescription drugs, some of which are prescribed inappropriately and without proper attention to side-effects2. Elderly people living in nursing homes are even more likely to receive medications and to experience side-effects3. Thus, in one year, 97% of elderly nursing home residents received a prescription drug, compared with 71% of patients living in the community4. Failure to identify side-effects can lead to use of other drugs to treat the symptoms, rather than adjustment of the dose of the drug responsible. Why do side-effects go unnoticed in elderly people? Older people often have low health expectations and are less likely to complain. Patients with cognitive impairment have difculties in communicating their discomfort; those living in nursing homes may rely on care staff to alert the physician to possible side-effects. Some side-effects can be mistaken for the effects of old age and age-related illness. This is particularly the case for anticholinergic side-effects, which are among the most common drug-related effects experienced by elderly people living in nursing and residential homes5,6. This review highlights the need for better understanding, assessment and management of anticholinergic side-effects in elderly people.
DRUGS WITH ANTICHOLINERGIC ACTIVITY
Peters5 identied 22 categories with signicant anticholinergic activity, including those with an anticholinergic
Box 1 Drugs with anticholinergic adverse effects used in the elderly
(Adapted from Refs 5 and 6)
Anticholinergic drugs Antiemetics/anti-vertigo Hyoscine, cyclizine, dimenhydrinate, meclozine, trimethobenzamide, promethazine, prochlorperazine Benztropine, biperiden, procyclidine, trihexyphenidyl, ethopropazine Belladonna alkaloids, clidinium bromide, dicycloverine, hyoscyamine, methscopolamine bromide, propantheline Oxybutynin, avoxate, dicyclomine Belladonna alkaloids Atropine solution, ipratropium Hyoscine, atropine Atropine solution, cyclopentolate, homatropine, tropicamide Disopyramide, procainamide, quinidine Diphenoxylate/atropine, tincture of belladonna Diphenhydramine, chlorphenamine, clemastine, dexchlorpheniramine, hydroxine, mepyramine (pyrilamine), promethazine Cyclobenzaprine, orphenadrine Propantheline Amitriptyline, imipramine, doxepin, trimipramine, nortriptyline, protriptyline, amoxapine, maprotiline, clomipramine Chlorpromazine, thioridazine, clozapine, uphenazine, prochlorperazine, thiothixene Glutethimide, pethidine Henbane, deadly nightshade
Antiparkinson
Antispasmodics (gastrointestinal)
Antispasmodics (genitourinary) Anti-migraine drugs Bronchodilators Pre-anaesthetics Mydriatics/cycloplegics
Drugs with anticholinergic side-effects Antiarryhthmics Antidiarrhoeals Antihistamines
Blazer et al.4 reported that, during one year, nearly 60% of nursing home residents had received drugs with anticholinergic (antimuscarinic) activity, compared with 23% of elderly people living in the community. The most frequently prescribed of these drugs were thioridazine, chlorpromazine and diphenoxylate/atropine. Several types of drug can cause anticholinergic side-effects (Box 1).
Medical University of South Carolina, Department of Psychiatry (PH-141), 67 President Street, PO Box 250861, Charleston, South Carolina, 29425, USA;
1
Skeletal muscle relaxants Anti-ulcer drugs Antidepressants
Antipsychotics
School of Psychiatry and Behavioural Sciences, University Hospital of South
Manchester, Manchester, UK Correspondence to: Professor Jacobo Mintzer E-mail: mintzerj@musc.edu
Miscellaneous Herbal medicines
REVIEW ARTICLES
457
Anticholinergic side-effects of drugs in elderly people
JOURNAL
OF
THE ROYAL
SOCIETY OF
MEDICINE
Volume
93
September
2000
Table 1 In-vitro anticholinergic activity (at 10 nmol/L) of the 25 medications most commonly prescribed to elderly people in the USA (Adapted from Ref. 7)
Detectable atropine-like activity (ranked from high to low) No detectable atropine-like activity
Cimetidine Prednisolone Theophylline Digoxin Nifedipine Frusemide Ranitidine Isosorbide dinitrate Warfarin Dipyridamole Codeine Dyazide Captopril
Hydrochlorothiazide Propranolol Salicyclic acid Nitroglycerin Insulin Methyldopa Ibuprofen Diltiazem Atenolol Metoprolol Timolol
does not always predict clinical effects; alternatively, the activity reported by Tune et al., though insufcient to cause obvious side-effects with cimetidine monotherapy in young adults, might be troublesome in those already receiving anticholinergic medications or otherwise vulnerable. High doses of cimetidine in elderly patients have occasionally been associated with reversible confusional states (confusion, delirium, slurred speech, hallucinations, coma8).
RECOGNIZING ANTICHOLINERGIC SIDE-EFFECTS
Symptoms which may be caused by drugs with anticholinergic activity include: . Dry or sticky lips; difculty beginning to speak (need to lick lips rst) . Urinary disorders, necessitating use of catheter . Skin dry, pale and cool . Insecure movement; falls without obvious reason, blurred vision . Increased anxiety, with rapid, shallow breathing, tachycardia, cardiac arrhythmias. Anticholinergic actions affect multiple systems, causing a range of peripheral and central side-effects and symptoms (Table 2). Central anticholinergic effects include memory decits, confusion and disorientation, agitation, hallucinations and delirium4,6. In the extreme, anticholinergic toxicity depresses brain function, with coma and circulatory collapse.
IMPACT OF ANTICHOLINERGIC SIDE-EFFECTS
458
mode of action (e.g. drugs for parkinsonism, irritable bowel syndrome, urinary incontinence) and others with unwanted anticholinergic effects. Tune et al.7 looked for in-vitro anticholinergic activity in the 25 drugs most commonly prescribed for elderly people and found such activity in 14 (Table 1). Often, elderly patients receive several such drugs simultaneously. Many non-prescription drugs have anticholinergic potential; this is true of the antihistamines in cold/u and hayfever treatmentse.g. diphenhydramine (Benylin Four Flu); triprolidine (Actifed); chlorpheniramine (Piriton/ Contact 400); and promethazine (Night Nurse/Phenergan). Skin creams and lotions also contain antihistaminese.g. diphenhydramine (Allereze cream) or mepyramine (Anthisan)and treatments for sleep disturbance include diphenhydramine (Nightcalm/Nytol) and promethazine (Sominex/Phenergan). Some hayfever medications contain theophylline (e.g. Chest-Eze), antidiarrhoeals include extract of belladonna (Enterosan, Opazimes) and some treatments for irritable bowel syndrome contain hyoscine (Buscopan). The number of drugs with anticholinergic potential available without prescription is increasing6, so that the use of such medications is becoming more difcult to monitor. For example, histamine H2 antagonists can be had over the counter for indigestioncimetidine (Tagamet/Acid-eze); ranitidine (Zantac); famotidine (Pepcid AC). Of those drugs examined by Tune et al.7, cimetidine had the highest anticholinergic activity in vitro, although side-effects attributed to this activity do not feature in the labelling of cimetidine. One interpretation is that in-vitro pharmacological activity
Why should old people be at increased risk of anticholinergic side-effects4,9? Part of the reason may lie in decient drug metabolism and elimination, as well as agerelated decits in cholinergic neurotransmission6. For people living in nursing homes, with little to distract them, side-effects can be particularly distressing and difcult to cope with. For example, dry mouth, while apparently trivial, can cause speech difculties, dental decay or trouble with dentures. Chewing and swallowing may become painful, and the patient may refuse solid food. The pain of dry mouth can be extremely distressing for older patients, who may become frustrated and agitated by an inability to communicate their distress. Older people often have multiple illnesses. In the USA as many as ve chronic conditions in one person is not unusual10, and conditions such as angina, congestive heart failure, constipation, diabetes mellitus, glaucoma, urinary dysfunction, sleep disturbance and dementia are all worsened by drugs with anticholinergic activity6. Pupillary dilatation and the inability to accommodate will impair near vision, thus increasing the risk of accidents, including falls,
JOURNAL OF
THE
ROYAL
SOCIETY
OF
MEDICINE
Volume 93
September 2000
Table 2 Spectrum of anticholinergic side-effects (Adapted from Ref. 6)
Mild Moderate Severe
Dryness of mouth (modest)
Moderately disturbing dry mouth/thirst Speech problems Reduced appetite
Difculty chewing, swallowing, speaking Impaired perception of taste and texture of food Mucosal damage Dental decay, periodontal disease, denture mist Malnutrition Respiratory infection Increased risk of accidents and falls, leading to decreased function Exacerbation/precipitation of acute angle closure glaucoma Faecal impaction (in patients with constipation) Altered absorption of concomitant medications Paralytic ileus, pseudo-obstruction Urinary retention, urinary tract infection (in patients with urinary hesitancy)
Mild dilatation of pupils
Inability to accommodate Vision disturbances Dizziness Oesophagitis Reduced gastric secretions, gastric emptying (atony) Reduced peristalsis, constipation
Urinary hesitancy Increased heart rate
Conduction disturbances, supraventricular tachyarrhythmias Exacerbation of angina Congestive heart failure Thermoregulatory impairment leading to hyperthermia (heatstroke)
Decreased sweating Drowsiness Fatigue Mild amnesia Inability to concentrate Excitement Restlessness Confusion Memory impairment
Profound restlessness and disorientation, agitation Hallucinations, delirium Ataxia, muscle twitching, hyperreexia, seizures Exacerbation of cognitive impairment (in patients with dementia)
and may precipitate narrow-angle glaucoma in predisposed patients. In patients with constipation, anticholinergic effects may lead to stomatitis, paralytic ileus or faecal impaction. Drug-induced increases in heart rate may worsen symptoms of angina, and inhibition of sweating may cause life-threatening hyperthermia. Patients with urinary hesitancy may experience urinary retention and urinary tract infection, a common cause of delirium. Men with prostatism are at high risk of acute urinary retention as an anticholinergic side-effect. Delirium can be caused by blockade of brain muscarinic receptors; drugs with anticholinergic activity are the most common cause of drug-induced delirium7,11. More than one-fth of elderly patients admitted to hospital develop delirium, particularly those with dementia and multiple illnesses. In patients with dementia, anticholinergic drugs further inhibit cognitive performance and counteract the benecial effects of cholinergic enhancers used to treat cognitive impairment. Williamson et al.9 examined the use of psychotropics and antiparkinsonian drugs (both have marked anticholinergic effects) in nearly 2000 patients admitted to geriatric units. More than a quarter were receiving one such drug, and 13% of those patients had signicant adverse
events6. Nevertheless, physicians often attribute anticholinergic symptoms in elderly people to ageing or agerelated illness rather than the effects of drugs6. Even physicians and carers who appreciate that such symptoms can be drug-induced may regard them as inevitable, simply because they are so common.
UNDERSTANDING THE RISK: POLYPHARMACY AND `ANTICHOLINERGIC LOAD'
In their nursing home study, Blazer et al.4 calculated that between 21% and 32% of residents could have been taking two or more drugs with anticholinergic activity (three or more drugs 1017% of patients; ve or more drugs, up to 5%). The most common combinations were thioridazine/ benzhexol and thioridazine/chlorpromazine (benzhexol is now seldom used). However, combined use of thioridazine and amitriptyline (each with marked anticholinergic activity) was also very common, demonstrating a lack of concern about combined anticholinergic effects. Partly through legislation, there have been reductions in the use in US nursing homes of psychotropic drugs, many of which have marked anticholinergic activity12. The availability of newer psychotropic drugs has also had an impact on prescribing by primary care physicians
459
JOURNAL
OF
THE ROYAL
SOCIETY OF
MEDICINE
Volume
93
September
2000
treating patients in nursing homes13. With increasing use of newer psychotropics anticholinergic side-effects in elderly people may be declining, but many different drugs have some anticholinergic activity and elderly patients receiving multiple drugs are still at risk of `anticholinergic load'14. In theory the physician can predict the anticholinergic load and the risk of side-effects associated with any combination of drugs. In practice, the information available from the product label and from the published work focuses on sideeffects of drugs used as monotherapy. The concept of anticholinergic load illustrates that side-effects can be caused by combinations of drugs, even if the individual drugs do not cause obvious side-effects.
PSYCHOTROPIC DRUGS: THE MAJOR BURDEN
These are among the most common medications taken by elderly people living in nursing homes (mainly antipsychotics, antidepressants and anxiolytics/sedatives). Spore et al.15 found that 43% of elderly patients in residential care were receiving psychotropic drugs. Antidepressants and antipsychotics have been linked most often with disorders due to anticholinergic activity.
Antidepressants
The use of antidepressants in elderly people requires particular care16,17. Tricyclic antidepressants (TCAs) have been in use for over 30 years, and imipramine and amitriptyline are the standard against which new drugs are evaluated. Old patients are more likely than young adults to experience side-effects with TCAs (see Box 1 for examples). Apart from the postural hypotension and sedation associated with the TCAs, anticholinergic sideeffects such as constipation, urinary retention and confusion are particular causes for concern. Some authorities have advised against the use of TCAs such as imipramine, amitriptyline and doxepin in the elderly because of their side-effects, not least their anticholinergic effects1820. Nortriptyline, lofepramine and desipramine (the least anticholinergic of the TCAs) tend to be better tolerated. Some newer antidepressants may be useful alternatives to TCAs in elderly people21. The selective serotonin reuptake inhibitors such as uoxetine and sertraline have been recommended, partly because of their relative freedom from anticholinergic side-effects19,20. Nefazodone, bupropion, venlafaxine and mirtazapine also have less anticholinergic potential than the older drugs22.
Antipsychotics
dementia2325, despite a lack of prospective placebocontrolled studies on their use in these circumstances26. Substantial differences exist between conventional neuroleptic drugs with respect to anticholinergic activity; chlorpromazine and thioridazine have the highest activity27,28 with considerable side-effects29 (see Box 1). Haloperidol has lower muscarinic afnity and the risk of anticholinergic side-effects is lower, but extrapyramidal symptoms are more troublesome29. Conventional neuroleptic drugs can also cause other side-effects. Low doses have been recommended for elderly patients, although this may limit the efcacy of these agents26. Novel antipsychotic drugs have been widely studied in younger patients (particularly those with schizophrenia), but for most drugs no controlled trials have been reported in elderly patients26. An exception is risperidone, which has been compared with placebo in two trials in elderly nursing home patients with dementia30,31. Risperidone is the only novel antipsychotic so far registered for this indication in certain countries (though not in the UK). It has no measurable anticholinergic activity28 and has not been reported to cause anticholinergic side-effects in elderly patients30,31. By contrast, clozapine has marked anticholinergic activity and is associated with profound anticholinergic side-effects3234. When clozapine (and other antipsychotics with high anticholinergic activity) are withdrawn, two types of withdrawal reaction are seen `cholinergic rebound', with nausea, vomiting, loss of appetite, malaise, diarrhoea, rhinorrhoea, sweating, anxiety, agitation and insomnia35,36; and movement disorders such as dyskinesia, akathisia and parkinsonism37. When switching patients to a drug with low anticholinergic potential, physicians sometimes mistake withdrawal symptoms for the side-effects of the new drug.
CHANGING PRESCRIBING PRACTICE
460
Conventional neuroleptic drugs are widely used in the treatment of behavioural and psychological symptoms of
Physicians should be alert to the possibility that dry mouth, constipation and blurred vision may be caused by medication. Changes in intellectual function should also be investigated, especially in patients who already have cognitive impairment. For patients in whom side-effects can have particularly unpleasant consequences (e.g. those with gastrointestinal disease, bladder neck obstruction, glaucoma, cardiac disease or cognitive impairment), serious consideration should be given to switching to a drug that lacks anticholinergic side-effects. For most drugs with anticholinergic potential an alternative is available. Combinations of drugs with strong anticholinergic activity, such as thioridazine and amitriptyline, should obviously be avoided. The use of drugs with minimal anticholinergic activity from the outset should avoid the need to switch medication (and the risk of
JOURNAL OF
THE
ROYAL
SOCIETY
OF
MEDICINE
Volume 93
September 2000
cholinergic rebound). If switching is necessary, the hazard of rebound can be lessened by slowly tapering the doses, with additional anticholinergic medication if necessary38. For patients already receiving treatment, the current anticholinergic load should always be considered before another drug is introduced. If the current load is high, even drugs with moderate or low anticholinergic activity may precipitate side-effects. No drug should be introduced without careful assessment of existing medications and symptoms. Often, there is little published information on the complex combinations of drugs used in elderly people. In-vitro activity can only be a broad predictor of clinical effects, and information from clinical trials may likewise be of limited value; for example, so far, trials of antipsychotic drugs in elderly people have not specically inquired about anticholinergic side-effects but have relied on spontaneous reporting by patients or carers. The range and severity of side-effects may therefore have been underestimated.
INFORMING PATIENTS AND CARERS
Informing patients and carers about potential side-effects is of great importance. Difculties with side-effects are likely to result in poorer treatment outcomes and are a major cause of non-compliance. If patients and carers are sensitively informed about unwanted effects, this will help to reduce the anxiety and distress that side-effects may cause.
PHYSICAL MEASURES
When anticholinergic side-effects do occur and the drug cannot be stopped, some steps can be taken to reduce their impact on the patient. The discomfort of dry mouth can be reduced by taking sips of water, or by chewing sugarless gum or soft sweets, while articial tears are useful for dry eyes. Pilocarpine solution has been used as a mouthwash for dry mouth or as eye drops for blurred vision39,40. Constipation can be reduced by high-bre diets, bre supplements, increased uid intake or greater patient mobility (e.g. walking down the ward to meals). Oral bethanechol, a cholinergic agonist, has been used to treat anticholinergic effects but can itself cause tremor, diarrhoea and abdominal cramps39. Furthermore, treatment of drug side-effects with another drug is not good practice; a much better strategy is to prescribe a medication relatively free from side-effects.
REFERENCES
1 Salom IL, Davis K. Prescribing for older patients: how to avoid toxic drug reactions. Geriatrics 1995;50:3740 2 Royal College of Physicians. Medication for Elderly People. London: RCP, 1997
3 Furniss L, Burns A, Craig S, Cooke J, Scobie S. The effect of a pharmacist's intervention in nursing and residential homes. Br J Psychiatry (in press) 4 Blazer DG, Federspiel CF, Ray WA, Schaffner W. The risk of anticholinergic toxicity in the elderly: a study of prescribing practices in two populations. J Gerontol 1983;38:315 5 Peters NL. Snipping the thread of life. Antimuscarinic side effects of medications in the elderly. Arch Intern Med 1989;149:241420 6 Feinberg M. The problems of anticholinergic adverse effects in older patients. Drugs Aging 1993;3:33548 7 Tune L, Carr S, Hoag E, Cooper T. Anticholinergic effects of drugs commonly prescribed for the elderly: potential means for assessing risk of delirium. Am J Psychiatry 1992;149:13934 8 Martindale the Extra Pharmacopeia. London: Pharmaceutical Press, 1989 9 Williamson J, Chopin JM. Adverse reactions to prescribed drugs in the elderly: a multicentre investigation. Age Ageing 1980;9:739 10 OTA Project Staff, Solan G, Behney C, et al. Prescription Drugs and Elderly Americans: Ambulatory Use and Approaches for Coverage for Medicare. Washington, DC: US Congress Ofce of Technology Assessment, Health Program, 1987 11 Jitapunkal S, Pillay I, Ebrahim S. Delirium in newly admitted elderly persons: a prospective study. Quart J Med 1992;83:30714 12 Rovner BW, Edelman BA, Cox MP, et al. The impact of antipsychotic drug regulations on psychotropic prescribing practices in nursing homes. Am J Psychiatry 1992;149:13902 13 Lasser RA, Sunderland T. Neuropsychotropic medication use in nursing home residents. J Am Geriatr Soc 1998;46:2027 14 Seifert R, Jamieson J, Gardner R. Use of anticholinergics in the nursing home: an empirical study. Drug Intell Clin Pharmacy 1983;17:4703 15 Spore D, Mor V, Larrat EP, Hiris J, Hawes C. Regulatory environment and psychotropic use in board-and-care facilities: results of a 10-state study. J Geront A Biol Sci Med Sci 1996; 51:M13141 16 Gerson SC, Plotkin DA, Jarvik LF. Antidepressant drug studies 1964 to 1986: empirical evidence for aging patients. J Clin Psychopharmacol 1998;8:31122 17 Alexopoulos GS. Treatment of depression. In: Salzman C, ed. Clinical Geriatric Psychopharmacology. Baltimore: Williams & Wilkins, 1992 18 Meyers BS, Kalayam B. Update in geriatric psychopharmacology. In: Billig N, Rabind PV, eds. Issues in Geriatric Psychiatry. Basel: Karger, 1989:11437 19 Preskorn SH. Recent pharmacologic advances in antidepressant therapy for the elderly. Am J Med 1993;94:2S12S 20 Salzman C. Pharmacologic treatment of depression in the elderly. J Clin Psychiatry1993;54:238 21 Katona CLE. New antidepressants in the elderly. In: Holmes, C, Howard R, eds. Advances in Old Age Psychiatry: Chromosomes to Community Care. Peterseld: Wrightson Biomedical Publishing, 1997;14360 22 Katona C, Livingston G, Manela M, et al. The symptomatology of depression in the elderly. Int J Psychopharmacol 1997;12(suppl 7):S1923 23 Yeager BF, Farnett LE, Ruzicka SA. Management of the behavioral manifestations of dementia. Arch Intern Med 1995;155:25060 24 Sunderland T. Treatment of the elderly suffering from psychosis and dementia. J Clin Psychiatry 1996;57(suppl 9):536 25 Herrmann N, Lanctot KL, Naranjo CA. Behavioral disorders in demented elderly patients: current issues in pharmacotherapy. CNS Drugs 1996;6:2180300 26 Stoppe G, Brandt CA, Staedt JH. Behavioural problems associated with dementia: the role of newer antipsychotics. Drugs Aging 1999;14:4154 27 Bolden C, Cusack B, Richelson E. Antagonism by antimuscarinic and neuroleptic compounds at the ve cloned human muscarinic cholinergic receptors expressed in Chinese hamster ovary cells. J Pharmacol Exp Ther 1992;260:57680
461
JOURNAL
OF
THE ROYAL
SOCIETY OF
MEDICINE
Volume
93
September
2000
28 Bymaster FP, Calligaro MS, Falcone JF, et al. Radioceptor binding prole of the atypical antipsychotic olazapine. Neuropsychopharmacology 1996;14:8796 29 Goff DC, Schader RI. Non-neurological side effects of antipsychotic agents. In: Hirsch SR, Weinberger DR, eds. Schizophrenia. Oxford: Blackwell Science, 1995:56684 30 Katz IR, Jeste DV, Mintzer JE, Clyde C, Napolitano J, Brecher M. Comparison of risperidone and placebo for psychosis and behavioural disturbances associated with dementia: a randomized, double-blind trial. Risperidone Study Group. J Clin Psychiatry 1999;60:10715 31 De Deyn PP, Rabberu K, Ramussen A, et al. A randomized trial of risperidone, placebo, and haloperidol for behavioral symptoms of dementia. Neurology 1999;53:94655 32 Kumar V. Use of atypical antidepressants in geriatric patients: a review. Int J Geriatr Psychopharmacol 1997;1:1523 33 Pitner JK, Mintzer JE, Pennypacker LC, Jackson CW. Efcacy and adverse effects of clozapine in four elderly psychotic patients. J Clin Psychiatry 1995;56:1805
34 Chengappa KN, Baker RW, Kreinbrook SB, Adair D. Clozapine use in female geriatric patients with psychoses. J Geriatr Psychiatr Neurol 1995; 8:125 35 Staedt J, Stoppe G, Hajak G, Ruther E. Rebound insomnia after abrupt clozapine withdrawal. Eur Arch Psychiatry Clin Neurosci 1996;246:7982 36 Durst R, Teitelbaum A, Katz G, Knobler HY. Withdrawal from clozapine: the ``rebound phenomenon''. Isr J Psychiatry Relat Sci 1999; 36:1228 37 Ahmed S, Chengappa KN, Naidu VR, Baker RW, Parepally H, Schooler NR. Clozapine withdrawal-emergent dystonias and dyskinesias: a case series. J Clin Psychiatry 1998;59:4727 38 Borison RL. Changing antipsychotic medication: guidelines on the transition to treatment with risperidone. The Consensus Study Group on Risperidone Dosing. Clin Ther 1996;18:592607 39 Ettinger RL. Xerostomia: a complication of ageing. Aust Dent J 1981; 1:11116 40 Baker KA, Ettinger RL. Intra-oral effects of drugs in elderly persons. Geridontics 1985;1:11116
462
You might also like
- Polypharmacy in The: The Bagful of Pills: ElderlyDocument34 pagesPolypharmacy in The: The Bagful of Pills: ElderlyrandatagNo ratings yet
- Case Study on Epilepsy Patient's Treatment and RecoveryDocument11 pagesCase Study on Epilepsy Patient's Treatment and RecoveryHarry Sivia100% (3)
- ObatDocument7 pagesObatMaria RudiNo ratings yet
- The Best Practice Is The Lowest Effective Dose Your Third Psychiatric Consultation: Diet, Exercise, and Sleep Trump Medications Medication is the Last Option Your Fourth Psychiatric ConsultationFrom EverandThe Best Practice Is The Lowest Effective Dose Your Third Psychiatric Consultation: Diet, Exercise, and Sleep Trump Medications Medication is the Last Option Your Fourth Psychiatric ConsultationNo ratings yet
- MCM16-283 Drug Induced DiseasesDocument128 pagesMCM16-283 Drug Induced DiseasesAshraf Khan ShaonNo ratings yet
- Dimenhydrinate injection summaryDocument8 pagesDimenhydrinate injection summarymayra chipanaNo ratings yet
- Rangkuman Book ReadingDocument7 pagesRangkuman Book ReadingBlackswannnNo ratings yet
- A Presentation On Adr Due To AntibioitcsDocument18 pagesA Presentation On Adr Due To AntibioitcsAnta SharmaNo ratings yet
- Pharmacology Sba AnswersDocument8 pagesPharmacology Sba AnswersMaria GillNo ratings yet
- Cortex Where Spread of SeizureDocument11 pagesCortex Where Spread of SeizureDustin JohnNo ratings yet
- DiphenhydramineDocument10 pagesDiphenhydramineFebry Dian SinagaNo ratings yet
- Antiemetics: Alcantara, Baarde, Daquer, MellomedaDocument11 pagesAntiemetics: Alcantara, Baarde, Daquer, MellomedaEduard100% (1)
- Toxic Effects of Drugs ExplainedDocument185 pagesToxic Effects of Drugs ExplainedAntonette Africa MercadoNo ratings yet
- DiphenhydramineDocument6 pagesDiphenhydramineParker LeethNo ratings yet
- Topic 8 - Management of Adverse Drug ReactionsDocument27 pagesTopic 8 - Management of Adverse Drug ReactionsPrincewill SmithNo ratings yet
- DRUG FILEDocument20 pagesDRUG FILESanjeevNo ratings yet
- HaloperidolDocument4 pagesHaloperidolNickol BaylonNo ratings yet
- Digestive System Diseases and Therapy NotesDocument19 pagesDigestive System Diseases and Therapy NotesMbah GapinbissiNo ratings yet
- Summary & Study Guide - Mind over Meds: When to Let Your Body Heal on Its OwnFrom EverandSummary & Study Guide - Mind over Meds: When to Let Your Body Heal on Its OwnNo ratings yet
- Chronic Urticaria and Treatment Options: Cme ArticleDocument8 pagesChronic Urticaria and Treatment Options: Cme ArticleYogi SanjayaNo ratings yet
- Calcium Carbonate for Bone HealthDocument14 pagesCalcium Carbonate for Bone HealthBianca Freya Porral85% (13)
- E-Therapeutics+ - Minor Ailments - Therapeutics - Central Nervous System Conditions - Vertigo and DizzinessDocument5 pagesE-Therapeutics+ - Minor Ailments - Therapeutics - Central Nervous System Conditions - Vertigo and DizzinessSamMansuriNo ratings yet
- Answer For Pharmacology Final ReviewDocument13 pagesAnswer For Pharmacology Final Reviewronon87No ratings yet
- Anti Psychotic DrugsDocument6 pagesAnti Psychotic DrugsJoseph NyirongoNo ratings yet
- ChemDocument10 pagesChemANJOSH 007No ratings yet
- Side Effects:: AtropineDocument7 pagesSide Effects:: AtropinekletadaNo ratings yet
- PoisoningDocument29 pagesPoisoningYohannes luelNo ratings yet
- Pycnogenol Consumer/Patient Information SheetDocument1 pagePycnogenol Consumer/Patient Information SheetDeboraNainggolanNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Endocrine Pharmacology by DR - Mayur SaytaDocument27 pagesEndocrine Pharmacology by DR - Mayur Saytasahilthakker2012No ratings yet
- N C by Dr. Mohamed Baraka: Ausea AND Vomiting Onstipation AND DiarrheaDocument72 pagesN C by Dr. Mohamed Baraka: Ausea AND Vomiting Onstipation AND DiarrheaIbrahim Mahmoud AliNo ratings yet
- Piriton Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Document4 pagesPiriton Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)May MethaweeNo ratings yet
- Generic Name, Dose, Indications, Side Effects, Nursing Care, Rationale, Patient Teaching (38Document7 pagesGeneric Name, Dose, Indications, Side Effects, Nursing Care, Rationale, Patient Teaching (38Joanna Marie Datahan EstomoNo ratings yet
- Adverse Drug ReactionDocument6 pagesAdverse Drug ReactionNunkoo RajNo ratings yet
- The Average Person Has 4 Health Issues and Takes 4 Prescription DrugsDocument10 pagesThe Average Person Has 4 Health Issues and Takes 4 Prescription DrugsNICOLAENo ratings yet
- Amitriptyline HCLDocument2 pagesAmitriptyline HCLGLen CaniedoNo ratings yet
- DrugsDocument7 pagesDrugsKevin TanNo ratings yet
- Onsult: Ementia Reatment PdateDocument5 pagesOnsult: Ementia Reatment PdateAxel Robinson HerreraNo ratings yet
- Silver Sulfadiazine Cream Prevents Burn InfectionsDrug NameDosageTherapeuticActionIndicationContraindicationAdverse EffectNursing ConsiderationDocument11 pagesSilver Sulfadiazine Cream Prevents Burn InfectionsDrug NameDosageTherapeuticActionIndicationContraindicationAdverse EffectNursing ConsiderationKristine ReyesNo ratings yet
- CHN Drug StudyDocument10 pagesCHN Drug StudyJoshua Cyryll ComiaNo ratings yet
- Complementary and Alternative Therapies and the Aging Population: An Evidence-Based ApproachFrom EverandComplementary and Alternative Therapies and the Aging Population: An Evidence-Based ApproachRating: 5 out of 5 stars5/5 (1)
- Geriatrics Department BookDocument69 pagesGeriatrics Department BookHazemAbu-BakrNo ratings yet
- Adrenocortical AgentsDocument8 pagesAdrenocortical AgentsKarina Madriaga100% (1)
- Theselectionof Antiepilepticdrugs Forthetreatmentof Epilepsyinchildren AndadultsDocument10 pagesTheselectionof Antiepilepticdrugs Forthetreatmentof Epilepsyinchildren AndadultsFaizan MazharNo ratings yet
- Pemakaian Antibiotik Polifarmasi Pada GeritariDocument37 pagesPemakaian Antibiotik Polifarmasi Pada GeritariShinta LissevaNo ratings yet
- Zyrtec: Tablet Core: Tablet CoatingDocument5 pagesZyrtec: Tablet Core: Tablet CoatingDwi WirastomoNo ratings yet
- AmoxicillinDocument2 pagesAmoxicillindheng05No ratings yet
- Unusual and Interesting Adverse Cutaneous Drug ReactionsDocument9 pagesUnusual and Interesting Adverse Cutaneous Drug ReactionsRizti RachmawatiNo ratings yet
- Adverse Drug Reactions ExplainedDocument108 pagesAdverse Drug Reactions ExplainedBinod Sah100% (2)
- Endocrinotox Vademecum: Homeopathic Regulation of The Neuroendocrine SystemDocument77 pagesEndocrinotox Vademecum: Homeopathic Regulation of The Neuroendocrine SystemlaviniagavrilaNo ratings yet
- Antiseizure age-WPS OfficeDocument15 pagesAntiseizure age-WPS Officermconvidhya sri2015No ratings yet
- S 000 LBLDocument27 pagesS 000 LBLDan Angelo Lawagan FloresNo ratings yet
- Common DrugsDocument138 pagesCommon DrugsDIPANJAN MAJUMDAR100% (19)
- Deanxit SPCDocument10 pagesDeanxit SPCXajepoxNo ratings yet
- B233 Exam 5test Mapfall2010Document5 pagesB233 Exam 5test Mapfall2010Katie L HollingsworthNo ratings yet
- Drug Card PhenytoinDocument5 pagesDrug Card PhenytoinGifther JohnNo ratings yet
- Drug StudyDocument24 pagesDrug StudyMc Joewell HudencialNo ratings yet
- Food and Drug InteractionsDocument16 pagesFood and Drug InteractionsSirijoti KanNo ratings yet
- Anti-Aging Therapeutics Volume XIIIFrom EverandAnti-Aging Therapeutics Volume XIIINo ratings yet
- Underage Marriage of Young Girls and Teenagers in AsiaDocument3 pagesUnderage Marriage of Young Girls and Teenagers in AsiaborninbrooklynNo ratings yet
- Warren Jeffs' Original IndictmentsDocument6 pagesWarren Jeffs' Original IndictmentsborninbrooklynNo ratings yet
- Transcript of Warren Jeffs Raping An Underage GirlDocument4 pagesTranscript of Warren Jeffs Raping An Underage Girlborninbrooklyn50% (2)
- 8.7.06 Audio Recording Transcript of Warren Jeffs Raping Merrianne, An Underage Girl From The FLDS Polygamy Group.Document4 pages8.7.06 Audio Recording Transcript of Warren Jeffs Raping Merrianne, An Underage Girl From The FLDS Polygamy Group.borninbrooklyn100% (2)
- Judge Shumate's Finding of Fact and Conclusion of LawDocument11 pagesJudge Shumate's Finding of Fact and Conclusion of LawborninbrooklynNo ratings yet
- Underage FLDS Marriages With Canadian Ties (Redacted)Document5 pagesUnderage FLDS Marriages With Canadian Ties (Redacted)borninbrooklynNo ratings yet
- Abbas Raptus: Incest in Mormon Fundamentalist CommunitiesDocument20 pagesAbbas Raptus: Incest in Mormon Fundamentalist CommunitiesborninbrooklynNo ratings yet
- Social Problems Associated With Polygamous vs. Monogamous MarriageDocument14 pagesSocial Problems Associated With Polygamous vs. Monogamous MarriageborninbrooklynNo ratings yet
- Janelle Brown Filing Against Bigamy Statutes of UtahDocument4 pagesJanelle Brown Filing Against Bigamy Statutes of UtahborninbrooklynNo ratings yet
- Warren Jeffs: Bigamous Marriages He Officiated or WitnessedDocument55 pagesWarren Jeffs: Bigamous Marriages He Officiated or Witnessedborninbrooklyn83% (6)
- Psychiatric Comorbidity in PedophilesDocument3 pagesPsychiatric Comorbidity in PedophilesborninbrooklynNo ratings yet
- Findings of Fact and Conclusions of Law On Consolidated Motion To Suppress YFZ Evidence 2009Document28 pagesFindings of Fact and Conclusions of Law On Consolidated Motion To Suppress YFZ Evidence 2009borninbrooklynNo ratings yet
- Women's Rights in Islam in Western SocietiesDocument300 pagesWomen's Rights in Islam in Western SocietiesborninbrooklynNo ratings yet
- CEDAW & Muslim Family Laws, in Search of Common Ground - Musawah Report, 2011Document87 pagesCEDAW & Muslim Family Laws, in Search of Common Ground - Musawah Report, 2011The Mossy BankNo ratings yet
- Control and Sexuality: Women's Rights and The Revival of Zina Law in Islamic SocietiesDocument258 pagesControl and Sexuality: Women's Rights and The Revival of Zina Law in Islamic SocietiesborninbrooklynNo ratings yet
- BROWN FAMILY SISTER WIVES Bankruptcies AnalysisDocument6 pagesBROWN FAMILY SISTER WIVES Bankruptcies AnalysisborninbrooklynNo ratings yet
- State of Texas 2nd Supplemental Witness List For The Trial of Warren JeffsDocument4 pagesState of Texas 2nd Supplemental Witness List For The Trial of Warren JeffsborninbrooklynNo ratings yet
- Federal Search Warrant For Red CadillacDocument10 pagesFederal Search Warrant For Red CadillacborninbrooklynNo ratings yet
- Judge Hyde's Order Denying Amended Motion To Recuse-1Document3 pagesJudge Hyde's Order Denying Amended Motion To Recuse-1borninbrooklynNo ratings yet
- Judge Hyde's Order Denying Amended Motion To Recuse Judge WaltherDocument3 pagesJudge Hyde's Order Denying Amended Motion To Recuse Judge WaltherborninbrooklynNo ratings yet
- Warren Jeffs' Original IndictmentsDocument6 pagesWarren Jeffs' Original IndictmentsborninbrooklynNo ratings yet
- State of Texas Witness List # 3Document2 pagesState of Texas Witness List # 3borninbrooklynNo ratings yet
- List # 2 of Witnesses For The State of Texas in The Trial of Warren JeffsDocument5 pagesList # 2 of Witnesses For The State of Texas in The Trial of Warren JeffsborninbrooklynNo ratings yet
- Expert Witness List For Warren Jeffs Texas TrialDocument2 pagesExpert Witness List For Warren Jeffs Texas Trialborninbrooklyn100% (1)
- State of Texas Witness Supoena List - Warrens Jeffs' WivesDocument6 pagesState of Texas Witness Supoena List - Warrens Jeffs' Wivesborninbrooklyn0% (1)
- Amended Motion For Rehearing On RecusalDocument47 pagesAmended Motion For Rehearing On RecusalborninbrooklynNo ratings yet
- Kody Brown Sister Wives Polygamy Lawsuit / Jonathan TurleyDocument39 pagesKody Brown Sister Wives Polygamy Lawsuit / Jonathan Turleyborninbrooklyn100% (1)
- Medications To Improve Cognitive Function in Traumatic Brain InjuryDocument89 pagesMedications To Improve Cognitive Function in Traumatic Brain InjuryborninbrooklynNo ratings yet
- Suprascapular Neuropathy in Volleyball Players: Original StudyDocument4 pagesSuprascapular Neuropathy in Volleyball Players: Original StudyborninbrooklynNo ratings yet
- A Critical Analysis of Relationship Marketing in Indian Pharmaceutical IndustryDocument12 pagesA Critical Analysis of Relationship Marketing in Indian Pharmaceutical IndustryRajeev ChinnappaNo ratings yet
- Monthly Activities Report 200 - 200: School Health Services ProgramDocument6 pagesMonthly Activities Report 200 - 200: School Health Services ProgramrahkelpNo ratings yet
- Reflection PaperDocument6 pagesReflection PapermarkNo ratings yet
- Internship Report OF Operation and Supply Chain Management of Eskayef Pharmaceuticals LimitedDocument96 pagesInternship Report OF Operation and Supply Chain Management of Eskayef Pharmaceuticals LimitedAminul Islam 2016209690No ratings yet
- Orientation To The IVT ProgramDocument16 pagesOrientation To The IVT ProgramCrystal Mae Castrodes DaquipilNo ratings yet
- Focus On Nursing Pharmacology Karch 5th Edition Test BankDocument36 pagesFocus On Nursing Pharmacology Karch 5th Edition Test Bankelapsionjealousymwhjl100% (38)
- Imidazole and Its Biological Activities A Review PDFDocument12 pagesImidazole and Its Biological Activities A Review PDFKim LunaNo ratings yet
- Case - Studies - in - Finance - Managing - For - Cor 2Document16 pagesCase - Studies - in - Finance - Managing - For - Cor 2Taylor StephensNo ratings yet
- Pharmaceutical Supply Chain in Vietnam Innovating Independent Community Pharmacy Services With SmartphonesDocument6 pagesPharmaceutical Supply Chain in Vietnam Innovating Independent Community Pharmacy Services With SmartphonesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pharmacuetics For The Students of Pharmacy Technicians (Category-B)Document45 pagesPharmacuetics For The Students of Pharmacy Technicians (Category-B)Naina's kitchencookingvediosNo ratings yet
- College of Pharmacy QA Unit: Course ILOS Classification Course Title: Code: 701507-2 Year/Level: 5/9Document10 pagesCollege of Pharmacy QA Unit: Course ILOS Classification Course Title: Code: 701507-2 Year/Level: 5/9hamam salih badriNo ratings yet
- Pharma Marketing KailasDocument167 pagesPharma Marketing KailasDhiraj ShuklaNo ratings yet
- 4.7 Ethylphenidate CritReviewDocument19 pages4.7 Ethylphenidate CritReviewkevinNo ratings yet
- HIRA ChecklistDocument27 pagesHIRA ChecklistAA T86% (7)
- Drug Nutrient InteractionDocument3 pagesDrug Nutrient InteractionAmira MNo ratings yet
- Square and Renata Ratio Analysis and ValuationDocument47 pagesSquare and Renata Ratio Analysis and ValuationRawkill 2000No ratings yet
- 1 s2.0 S0048969722084431 Main 1Document14 pages1 s2.0 S0048969722084431 Main 1Ram PrasathNo ratings yet
- Tieng Anh 4Document5 pagesTieng Anh 4Trần Thị Kiều TrangNo ratings yet
- Ethical Decision MakingDocument22 pagesEthical Decision MakingOmar ThanoonNo ratings yet
- Essay About The Great DepressionDocument6 pagesEssay About The Great DepressionafabittrfNo ratings yet
- Forensic Pharmacy and Forensic PharmacistDocument17 pagesForensic Pharmacy and Forensic PharmacistHajra Mehar100% (1)
- Therapeutic Classification of DrugsDocument4 pagesTherapeutic Classification of Drugslyn lynNo ratings yet
- PHARMA Industry Overview PresentationDocument27 pagesPHARMA Industry Overview PresentationdishaNo ratings yet
- How to Deal with Rising Oil Prices EfficientlyDocument17 pagesHow to Deal with Rising Oil Prices EfficientlyDishant Monga100% (1)
- Brazilian Pharmacopoeia: 6 EditionDocument893 pagesBrazilian Pharmacopoeia: 6 Editionchi nguyenNo ratings yet
- BS Pharm 1 Course SyllabusDocument2 pagesBS Pharm 1 Course SyllabusMarecar100% (2)
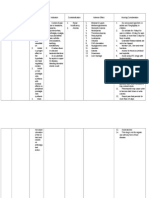
- Assessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation GoalDocument2 pagesAssessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation GoalI Am SmilingNo ratings yet
- Chapter 3 Pharmaceutical MarketingDocument50 pagesChapter 3 Pharmaceutical MarketingMark Tristan Asuncion100% (1)
- Common Medical NotationsDocument3 pagesCommon Medical NotationssaltarisNo ratings yet
- Clinical PharmacyDocument26 pagesClinical PharmacyboyapallymeghanaNo ratings yet