You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- There Will Come Soft RainsDocument8 pagesThere Will Come Soft RainsEng ProfNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- 1973 Further Discussion of Fiedler's Contingency Model of Leadership EffectivenessDocument8 pages1973 Further Discussion of Fiedler's Contingency Model of Leadership EffectivenesslengocthangNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- A Short Survey On Memory Based RLDocument18 pagesA Short Survey On Memory Based RLcnt dvsNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- MPI Unit 4Document155 pagesMPI Unit 4Dishant RathiNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Agma MachineDocument6 pagesAgma Machinemurali036No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Entrepreneurial Capacity Building: A Study of Small and Medium Family-Owned Enterprisesin PakistanDocument3 pagesEntrepreneurial Capacity Building: A Study of Small and Medium Family-Owned Enterprisesin PakistanMamoonaMeralAysunNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Department of Ece, Adhiparasakthi College of Engineering, KalavaiDocument31 pagesDepartment of Ece, Adhiparasakthi College of Engineering, KalavaiGiri PrasadNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Civil Rights Vocabulary Lesson PlanDocument4 pagesCivil Rights Vocabulary Lesson PlanKati ArmstrongNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
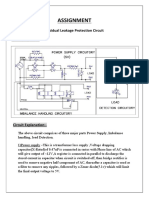
- Assignment: Residual Leakage Protection Circuit Circuit DiagramDocument2 pagesAssignment: Residual Leakage Protection Circuit Circuit DiagramShivam ShrivastavaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- TM Mic Opmaint EngDocument186 pagesTM Mic Opmaint Engkisedi2001100% (2)
- DLP English 10 AIRADocument8 pagesDLP English 10 AIRAMae Mallapre100% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Multiple Choice Practice Questions For Online/Omr AITT-2020 Instrument MechanicDocument58 pagesMultiple Choice Practice Questions For Online/Omr AITT-2020 Instrument Mechanicمصطفى شاكر محمودNo ratings yet
- CHAPTER 2 Part2 csc159Document26 pagesCHAPTER 2 Part2 csc159Wan Syazwan ImanNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- CIPD L5 EML LOL Wk3 v1.1Document19 pagesCIPD L5 EML LOL Wk3 v1.1JulianNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Internal Resistance To Corrosion in SHS - To Go On WebsiteDocument48 pagesInternal Resistance To Corrosion in SHS - To Go On WebsitetheodorebayuNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- 147 Amity Avenue Nampa, ID 81937 (999) 999-9999 William at Email - ComDocument4 pages147 Amity Avenue Nampa, ID 81937 (999) 999-9999 William at Email - ComjeyesbelmenNo ratings yet
- Hofstede's Cultural DimensionsDocument35 pagesHofstede's Cultural DimensionsAALIYA NASHATNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Topic: Grammatical Issues: What Are Parts of Speech?Document122 pagesTopic: Grammatical Issues: What Are Parts of Speech?AK AKASHNo ratings yet
- Government Hazi Muhammad Mohsin College Chattogram: Admission FormDocument1 pageGovernment Hazi Muhammad Mohsin College Chattogram: Admission FormThe Helper SoulNo ratings yet
- WWW Ranker Com List Best-Isekai-Manga-Recommendations Ranker-AnimeDocument8 pagesWWW Ranker Com List Best-Isekai-Manga-Recommendations Ranker-AnimeDestiny EasonNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Unit 2: Air Intake and Exhaust SystemsDocument10 pagesUnit 2: Air Intake and Exhaust SystemsMahmmod Al-QawasmehNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Atoma Amd Mol&Us CCTK) : 2Nd ErmDocument4 pagesAtoma Amd Mol&Us CCTK) : 2Nd ErmjanviNo ratings yet
- 53 English Work Book XDocument292 pages53 English Work Book XArun DhawanNo ratings yet
- Class 12 Physics Derivations Shobhit NirwanDocument6 pagesClass 12 Physics Derivations Shobhit Nirwanaastha.sawlaniNo ratings yet
- 12 Step Worksheet With QuestionsDocument26 pages12 Step Worksheet With QuestionsKristinDaigleNo ratings yet
- Work Energy Power SlidesDocument36 pagesWork Energy Power Slidessweehian844100% (1)
- Ultra Electronics Gunfire LocatorDocument10 pagesUltra Electronics Gunfire LocatorPredatorBDU.comNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- SDS ERSA Rev 0Document156 pagesSDS ERSA Rev 0EdgarVelosoCastroNo ratings yet
- A202 KBK3043 - Assignment Individual (20%) Review LiteratureDocument5 pagesA202 KBK3043 - Assignment Individual (20%) Review LiteratureAlfie AliNo ratings yet
- Moral GPS: A Positive Ethic For Our Multicultural WorldDocument279 pagesMoral GPS: A Positive Ethic For Our Multicultural WorldLeonard Bowman75% (4)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)