You might also like
- Detection of Vancomycin MIC by Agar Dilution in Clinical IsolateDocument11 pagesDetection of Vancomycin MIC by Agar Dilution in Clinical IsolateVamsi KrishnaNo ratings yet
- Himartshu MethodDocument5 pagesHimartshu MethodNiveditha NagasundaramNo ratings yet
- Prevalence of Methicillinresistant Staphylococcus Aureus Andor Intermediate Susceptibility To Vancomycin Isolated From PDocument7 pagesPrevalence of Methicillinresistant Staphylococcus Aureus Andor Intermediate Susceptibility To Vancomycin Isolated From Pعالمي الجميلNo ratings yet
- JCDR 7 1339Document4 pagesJCDR 7 1339RahayuNo ratings yet
- Jurnal Mikro 1Document6 pagesJurnal Mikro 1Elang SudewaNo ratings yet
- Risk Profile and Antimicrobial Susceptibility Pattern of Acinetobacter Baumanniiclinical Isolates in A Teaching Hospital in HyderabadDocument8 pagesRisk Profile and Antimicrobial Susceptibility Pattern of Acinetobacter Baumanniiclinical Isolates in A Teaching Hospital in HyderabadIJAR JOURNALNo ratings yet
- Vancomycin Resistance Among Isolates in A Rural Setting, EgyptDocument6 pagesVancomycin Resistance Among Isolates in A Rural Setting, EgyptRidho WahyutomoNo ratings yet
- Linezolida NovoDocument6 pagesLinezolida NovoGabriel EstevesNo ratings yet
- Van B Positive Vancomycin - Resistant Staphylococcus Aureus Among Clinical Isolates in Shendi City, Northern SudanDocument5 pagesVan B Positive Vancomycin - Resistant Staphylococcus Aureus Among Clinical Isolates in Shendi City, Northern SudanInternational Organization of Scientific Research (IOSR)No ratings yet
- Journal of Clinical Immunology and MicrobiologyDocument10 pagesJournal of Clinical Immunology and MicrobiologyAthenaeum Scientific PublishersNo ratings yet
- 2016, MDR and XDR, Basak, J PathogensDocument6 pages2016, MDR and XDR, Basak, J PathogensDrAhmedSalimNo ratings yet
- 1 s2.0 S1201971209000435 MainDocument7 pages1 s2.0 S1201971209000435 MainGopalaKrishnanNo ratings yet
- 86-Article Text-1486-2-10-20091026Document4 pages86-Article Text-1486-2-10-20091026adelNo ratings yet
- Antibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHDocument5 pagesAntibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHzia ul RahmanNo ratings yet
- Detection of Methicillin Resistance in Staphylococcus Species From Clinical SamplesDocument6 pagesDetection of Methicillin Resistance in Staphylococcus Species From Clinical SamplesOpenaccess Research paperNo ratings yet
- GeptodacinDocument6 pagesGeptodacinRubí YeverinoNo ratings yet
- Bangl. J. Vet. Med. (2008) - 6 (1) : 121-126: Staphylococcus Aureus (MRSA)Document6 pagesBangl. J. Vet. Med. (2008) - 6 (1) : 121-126: Staphylococcus Aureus (MRSA)noor_nordin_16No ratings yet
- Antibiotic Susceptibility Profile and Prevalence of AmpC Among Clinical Bacterial Isolates Obtained From Northwestern NigeriaDocument9 pagesAntibiotic Susceptibility Profile and Prevalence of AmpC Among Clinical Bacterial Isolates Obtained From Northwestern NigeriaUMYU Journal of Microbiology Research (UJMR)No ratings yet
- Isolation and Identification of Methicillin Resistance Staphylococcus Aureus From Clinical Samples and Their Drug Resistance PatternsDocument6 pagesIsolation and Identification of Methicillin Resistance Staphylococcus Aureus From Clinical Samples and Their Drug Resistance PatternsPaige MunroeNo ratings yet
- Prevalence and Antimicrobial Resistance Pattern of Methicillin Resistant Staphylococcus Aureus (MRSA) Strains..Document7 pagesPrevalence and Antimicrobial Resistance Pattern of Methicillin Resistant Staphylococcus Aureus (MRSA) Strains..Andi EsSeNo ratings yet
- Prevalence of Multidrug Resistance in Streptococcus Pyogenes Isolates From Different Clinical Sources in Al-Diwaniyah CityDocument9 pagesPrevalence of Multidrug Resistance in Streptococcus Pyogenes Isolates From Different Clinical Sources in Al-Diwaniyah CityCentral Asian StudiesNo ratings yet
- Cjim 7 114Document6 pagesCjim 7 114Fi NoNo ratings yet
- Journal of Clinical Immunology & MicrobiologyDocument9 pagesJournal of Clinical Immunology & MicrobiologyAthenaeum Scientific PublishersNo ratings yet
- Antimicrobial Susceptibility Pattern of Staphylococcus Aureus Isolated From Various Clinical Samples in A Tertiary Care HospitalDocument8 pagesAntimicrobial Susceptibility Pattern of Staphylococcus Aureus Isolated From Various Clinical Samples in A Tertiary Care HospitalIJAR JOURNALNo ratings yet
- The Emergence of Antibiotic Resistant Staphylococcus Aureusin Hospital Sewage A Threat To Public HealthDocument3 pagesThe Emergence of Antibiotic Resistant Staphylococcus Aureusin Hospital Sewage A Threat To Public HealthInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Resistance To Antifungal Agents: Mechanisms and Clinical ImpactDocument9 pagesResistance To Antifungal Agents: Mechanisms and Clinical ImpactAhmad BukhariNo ratings yet
- Rakhshanda Erum OADocument6 pagesRakhshanda Erum OAWijaya BudiNo ratings yet
- QC and Guideline BMD For AND Against MoldDocument3 pagesQC and Guideline BMD For AND Against MoldĐặng Thị Kim NgânNo ratings yet
- Mendes 2014Document7 pagesMendes 2014Sergei VoychukNo ratings yet
- MRSADocument6 pagesMRSAIgnacio Velasquez MiñoNo ratings yet
- MecC VitekDocument3 pagesMecC VitekmotibaNo ratings yet
- Microbiological Effects of Prior Vancomycin Use in Patients With Methicillin-Resistant Staphylococcus Aureus BacteraemiaDocument6 pagesMicrobiological Effects of Prior Vancomycin Use in Patients With Methicillin-Resistant Staphylococcus Aureus Bacteraemiaapi-19597023No ratings yet
- Articulo Evaluacion Final Antimicrobianos 1 2020Document9 pagesArticulo Evaluacion Final Antimicrobianos 1 2020Juan BojacaNo ratings yet
- Cinnamaldehyde Inhibits MRSA Biofilm Formation and Reduces Cell ViabilityDocument5 pagesCinnamaldehyde Inhibits MRSA Biofilm Formation and Reduces Cell Viabilitytuanda222No ratings yet
- Bacterial Contamination On Used Face Masks in Healthcare PersonnelDocument2 pagesBacterial Contamination On Used Face Masks in Healthcare PersonnelMaryam birmahNo ratings yet
- Osteomyelitis JournalDocument7 pagesOsteomyelitis JournalAmalia Dwi AryantiNo ratings yet
- Methicillin-Resistant Staphylococcus Aureus in NepDocument5 pagesMethicillin-Resistant Staphylococcus Aureus in NepHafiza AyeshaNo ratings yet
- MRSA Infection Trends in a Malaysian HospitalDocument6 pagesMRSA Infection Trends in a Malaysian HospitalZUKHRUFIA ISNA PRAMADEWINo ratings yet
- Wound Infections and MRSA: Marvin J. Bittner MDDocument93 pagesWound Infections and MRSA: Marvin J. Bittner MDOsama HassanNo ratings yet
- Characteristics of Community-And Hospital - Acquired Meticillin-Resistant Staphylococcus Aureus Strains Carrying Sccmec Type Iv Isolated in MalaysiaDocument6 pagesCharacteristics of Community-And Hospital - Acquired Meticillin-Resistant Staphylococcus Aureus Strains Carrying Sccmec Type Iv Isolated in Malaysiabenny christantoNo ratings yet
- Evaluation of Susceptibility Profiles of Some Bacteria To Flouroquinolones in Kano Metropolis, NigeriaDocument5 pagesEvaluation of Susceptibility Profiles of Some Bacteria To Flouroquinolones in Kano Metropolis, NigeriaUMYU Journal of Microbiology Research (UJMR)No ratings yet
- Antimicrob. Agents Chemother. 2008 Morozumi 348 50Document3 pagesAntimicrob. Agents Chemother. 2008 Morozumi 348 50Accel XtremeNo ratings yet
- Dipakai Parry Et Al CiprofloxacinDocument8 pagesDipakai Parry Et Al CiprofloxacinratihNo ratings yet
- Saureus Meti RDocument6 pagesSaureus Meti RShi-Long LoiNo ratings yet
- Isolation, Identification and Antibiogram of Coagulase Negative Tertiary Care Teaching Hospital, Jaipur, IndiaDocument12 pagesIsolation, Identification and Antibiogram of Coagulase Negative Tertiary Care Teaching Hospital, Jaipur, IndiadrpklalNo ratings yet
- Multidrug Resistant Uropathogens in Urinary Tract Infections and Their Antibiotic Susceptibility PatternsDocument4 pagesMultidrug Resistant Uropathogens in Urinary Tract Infections and Their Antibiotic Susceptibility PatternsCERCEL ALESIA IOANANo ratings yet
- 1 s2.0 S1684118222001505 MainDocument7 pages1 s2.0 S1684118222001505 MainMohamed SalahNo ratings yet
- Community Acquired Mrsa: Pisespong Patamasucon, M.D. Pediatric Infectious Disease UNSOM - Las VegasDocument48 pagesCommunity Acquired Mrsa: Pisespong Patamasucon, M.D. Pediatric Infectious Disease UNSOM - Las VegasRashed NazzalNo ratings yet
- 491 PDFDocument4 pages491 PDFYashaswiniTateneniNo ratings yet
- 23 Lakshmi Et AlDocument4 pages23 Lakshmi Et AleditorijmrhsNo ratings yet
- BMC Research NotesDocument6 pagesBMC Research NotesShyam MishraNo ratings yet
- Methicillin-Resistant Staphylococcus Aureus: Comparison of Susceptibility Testing Methods and Analysis ofDocument6 pagesMethicillin-Resistant Staphylococcus Aureus: Comparison of Susceptibility Testing Methods and Analysis ofNguyễn Đức LongNo ratings yet
- Characteristics of Microbial Drug Resistance and Its Correlates in Chronic Diabetic Foot Ulcer InfectionsDocument9 pagesCharacteristics of Microbial Drug Resistance and Its Correlates in Chronic Diabetic Foot Ulcer InfectionsPutri Alif PermatasariNo ratings yet
- Clindamicina (Inglés)Document6 pagesClindamicina (Inglés)Gonzalo Daniel Llarrull BatistaNo ratings yet
- XXXXXXXXXXX BGDocument5 pagesXXXXXXXXXXX BGProbioticsAnywhereNo ratings yet
- hVISa y VISA 2007 PDFDocument9 pageshVISa y VISA 2007 PDFGustavo UrriagoNo ratings yet
- Molecular Identification of S. aureus and Resistance to Fusidic AcidDocument7 pagesMolecular Identification of S. aureus and Resistance to Fusidic AcidAna Milena Gutierrez PinedaNo ratings yet
- Susceptibility of Gram-Positive Cocci From 25 UK Hospitals To Antimicrobial Agents Including LinezolidDocument0 pagesSusceptibility of Gram-Positive Cocci From 25 UK Hospitals To Antimicrobial Agents Including LinezolidGabriel MataNo ratings yet
- Species Identification and Antifungal Susceptibility of Uncommon Blood Yeast IsolatesDocument8 pagesSpecies Identification and Antifungal Susceptibility of Uncommon Blood Yeast Isolatesa.rahadianNo ratings yet
- 1) StaphylococciDocument13 pages1) StaphylococciOmar K. FahmyNo ratings yet
- Mikrobiologi Dasar (DR - Latre)Document50 pagesMikrobiologi Dasar (DR - Latre)wawanNo ratings yet
- Streptococcus PyogenesDocument21 pagesStreptococcus PyogenesSakil MunnaNo ratings yet
- Etiological Spectrum and Antimicrobial Resistance Among Bacterial Pathogen Association With Urinary Tract Infection in Wasit Governorate/ IraqDocument11 pagesEtiological Spectrum and Antimicrobial Resistance Among Bacterial Pathogen Association With Urinary Tract Infection in Wasit Governorate/ IraqCentral Asian StudiesNo ratings yet
- Toxic Bacteria: By: Camilo, Lizette Joy CDocument21 pagesToxic Bacteria: By: Camilo, Lizette Joy CLizette Joy Cuilan-CamiloNo ratings yet
- Vibrio CholeraeDocument20 pagesVibrio CholeraeBernadette BeltranNo ratings yet
- Lab 3 - Smear Preparation Simple Staining and Gram StainingDocument29 pagesLab 3 - Smear Preparation Simple Staining and Gram StainingAyman ElkenawyNo ratings yet
- Anaerobic Bacteria QuizletDocument6 pagesAnaerobic Bacteria QuizletReca Marie FRIASNo ratings yet
- Streptococcus ThermophilusDocument4 pagesStreptococcus ThermophilusMeyta Chita II0% (1)
- The New Microbiology - From Microbiomes To CRISPRDocument205 pagesThe New Microbiology - From Microbiomes To CRISPRalery ahreallyNo ratings yet
- Adoc - Pub Formulasi Yoghurt Sinbiotik Dengan Penambahan PureDocument83 pagesAdoc - Pub Formulasi Yoghurt Sinbiotik Dengan Penambahan PureGemios24No ratings yet
- Certification: Performance TestedDocument7 pagesCertification: Performance TestedAbdulrahmanNo ratings yet
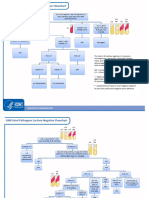
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- Microbiology Guide to Bacteriology C/S, Gram Stain, Skin Flora & StaphylococciDocument50 pagesMicrobiology Guide to Bacteriology C/S, Gram Stain, Skin Flora & Staphylococciakhir0% (1)
- KlebsiellaDocument3 pagesKlebsiellaFATHIMA ANo ratings yet
- Laboratory Diagnosis in Infections Produced by Anaerobic BacteriaDocument43 pagesLaboratory Diagnosis in Infections Produced by Anaerobic Bacteriarikirdn27No ratings yet
- Actinomycetes: Gram-positive filamentous bacteriaDocument18 pagesActinomycetes: Gram-positive filamentous bacteriayota_ahlyNo ratings yet
- CDC 2019 Report on Antibiotic Resistance ThreatsDocument8 pagesCDC 2019 Report on Antibiotic Resistance ThreatsmateNo ratings yet
- Introduction to EnterobacteriaceaeDocument33 pagesIntroduction to EnterobacteriaceaeМария М.No ratings yet
- Lecture (3) : Bacterial Cell StructureDocument47 pagesLecture (3) : Bacterial Cell StructureDrYahia Al-Qoa'fyNo ratings yet
- Microbiology Case StudyDocument3 pagesMicrobiology Case StudyPia Rose BaguioNo ratings yet
- A Hue of BluDocument24 pagesA Hue of Bluamonalemona11No ratings yet
- Dichotomous Key SampleDocument1 pageDichotomous Key SampleGerald ShouNo ratings yet
- SOCRANSKY 2002 - Dental Biofilms Difficult Therapeutic TargetsDocument44 pagesSOCRANSKY 2002 - Dental Biofilms Difficult Therapeutic TargetsLuiz Guilherme FiorinNo ratings yet
- The Structure and Functions of a Bacteria CellDocument16 pagesThe Structure and Functions of a Bacteria CellAngelo CalloNo ratings yet
- Student M10 Independent Identification of Unknown Bacteria and Automation.Document7 pagesStudent M10 Independent Identification of Unknown Bacteria and Automation.Gerald SorianoNo ratings yet
- Horizontal Gene Transfer in BacteriaDocument11 pagesHorizontal Gene Transfer in BacteriaAlejandra arecasNo ratings yet
- All BacteriaDocument14 pagesAll Bacteriamorale28100% (2)
- Vitek MS Guide to Bacteria and Yeast IDDocument19 pagesVitek MS Guide to Bacteria and Yeast IDS ONo ratings yet
- KEMAPUAN PEMBENTUKAN SLIME PADA STAPHYLOCOCCUSDocument9 pagesKEMAPUAN PEMBENTUKAN SLIME PADA STAPHYLOCOCCUSShofia hilwaNo ratings yet