You might also like
- 500 Free New Fullz ?Document555 pages500 Free New Fullz ?Mo Ar89% (28)
- Chart of Who Owns The Federal ReserveDocument9 pagesChart of Who Owns The Federal ReserveSUPPRESS THIS100% (6)
- Think Together 2101 E 4Th ST B Suite 200 Santa Ana, Ca 92705Document1 pageThink Together 2101 E 4Th ST B Suite 200 Santa Ana, Ca 92705Humayon MalekNo ratings yet
- IRS Form 56 (Notice Concerning Fiduciary Relationship)Document2 pagesIRS Form 56 (Notice Concerning Fiduciary Relationship)Benne James100% (6)
- Current Pay Statement: This Is A Statement of Earnings and Deductions. This Pay Statement Is Non-NegotiableDocument1 pageCurrent Pay Statement: This Is A Statement of Earnings and Deductions. This Pay Statement Is Non-Negotiablekevin kuhnNo ratings yet
- CPA Exam REG - S-Corporation Taxation.Document2 pagesCPA Exam REG - S-Corporation Taxation.Manny MarroquinNo ratings yet
- Statement of Earning & Deductions: Congo BomokoDocument4 pagesStatement of Earning & Deductions: Congo BomokoKeller Brown JnrNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- DOL RDWSU 2020 Form 5500Document205 pagesDOL RDWSU 2020 Form 5500seanredmondNo ratings yet
- CIR v. AlgueDocument2 pagesCIR v. AlgueRaish RojasNo ratings yet
- Miscellaneous Information: Copy B For RecipientDocument4 pagesMiscellaneous Information: Copy B For RecipientAubree Gates100% (1)
- Union Security Trust Fund 2007Document10 pagesUnion Security Trust Fund 2007Latisha WalkerNo ratings yet
- Tratamentul Total Al CanceruluiDocument71 pagesTratamentul Total Al CanceruluiAntal98% (98)
- Attention:: WWW - Efast.dol - GovDocument4 pagesAttention:: WWW - Efast.dol - GovIRSNo ratings yet
- Attention:: WWW - Efast.dol - GovDocument5 pagesAttention:: WWW - Efast.dol - GovIRSNo ratings yet
- Attention:: WWW - Efast.dol - GovDocument4 pagesAttention:: WWW - Efast.dol - GovIRSNo ratings yet
- US Internal Revenue Service: f5500sb - 1999Document8 pagesUS Internal Revenue Service: f5500sb - 1999IRSNo ratings yet
- US Internal Revenue Service: f5500sr - 1999Document2 pagesUS Internal Revenue Service: f5500sr - 1999IRSNo ratings yet
- US Internal Revenue Service: f5500sb - 2003Document7 pagesUS Internal Revenue Service: f5500sb - 2003IRSNo ratings yet
- US Internal Revenue Service: f5500sr - 2000Document2 pagesUS Internal Revenue Service: f5500sr - 2000IRSNo ratings yet
- US Internal Revenue Service: f5500sr - 2001Document2 pagesUS Internal Revenue Service: f5500sr - 2001IRSNo ratings yet
- US Internal Revenue Service: f5500sf - 1999Document1 pageUS Internal Revenue Service: f5500sf - 1999IRSNo ratings yet
- US Internal Revenue Service: f5500 - 2001Document4 pagesUS Internal Revenue Service: f5500 - 2001IRSNo ratings yet
- US Internal Revenue Service: f5500sr - 2003Document2 pagesUS Internal Revenue Service: f5500sr - 2003IRSNo ratings yet
- US Internal Revenue Service: F5500sa - 1999Document6 pagesUS Internal Revenue Service: F5500sa - 1999IRSNo ratings yet
- US Internal Revenue Service: F5500ssa - 1999Document2 pagesUS Internal Revenue Service: F5500ssa - 1999IRSNo ratings yet
- US Internal Revenue Service: f5500st - 1999Document2 pagesUS Internal Revenue Service: f5500st - 1999IRSNo ratings yet
- US Internal Revenue Service: f5500 - 2002Document6 pagesUS Internal Revenue Service: f5500 - 2002IRSNo ratings yet
- Attention:: WWW - Efast.dol - GovDocument8 pagesAttention:: WWW - Efast.dol - GovIRSNo ratings yet
- US Internal Revenue Service: f5500sp - 1999Document1 pageUS Internal Revenue Service: f5500sp - 1999IRSNo ratings yet
- US Internal Revenue Service: F5500se - 1999Document3 pagesUS Internal Revenue Service: F5500se - 1999IRSNo ratings yet
- US Internal Revenue Service: f5500sp - 2000Document1 pageUS Internal Revenue Service: f5500sp - 2000IRSNo ratings yet
- Filing PDFDocument82 pagesFiling PDFjgalenNo ratings yet
- Netflix 401 (K) PlanDocument51 pagesNetflix 401 (K) PlanoaifoiweuNo ratings yet
- Retirement Plan of Trustees 2007Document14 pagesRetirement Plan of Trustees 2007Latisha WalkerNo ratings yet
- Retirement & Pension Plan For NYCDCC Employees 2006Document13 pagesRetirement & Pension Plan For NYCDCC Employees 2006Latisha WalkerNo ratings yet
- F 5500 SsaDocument3 pagesF 5500 SsaIRSNo ratings yet
- Attention:: WWW - Efast.dol - GovDocument5 pagesAttention:: WWW - Efast.dol - GovIRSNo ratings yet
- US Internal Revenue Service: f5500 - 1995Document6 pagesUS Internal Revenue Service: f5500 - 1995IRSNo ratings yet
- Mercury NewsDocument87 pagesMercury NewskmccoynycNo ratings yet
- Carpenters Annuity Fund 2007Document19 pagesCarpenters Annuity Fund 2007Latisha WalkerNo ratings yet
- Retirement & Pension Plan For NYCDCC Employees 2007Document13 pagesRetirement & Pension Plan For NYCDCC Employees 2007Latisha WalkerNo ratings yet
- Carpenters Annuity Fund 2006Document20 pagesCarpenters Annuity Fund 2006Latisha WalkerNo ratings yet
- US Internal Revenue Service: F5500si - 2002Document6 pagesUS Internal Revenue Service: F5500si - 2002IRSNo ratings yet
- 2007 Form 5500 Carpenter Pension PlanDocument21 pages2007 Form 5500 Carpenter Pension PlanLatisha WalkerNo ratings yet
- US Internal Revenue Service: F5500si - 2003Document3 pagesUS Internal Revenue Service: F5500si - 2003IRSNo ratings yet
- Retirement Plan of Trustees 2006Document13 pagesRetirement Plan of Trustees 2006Latisha WalkerNo ratings yet
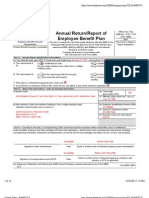
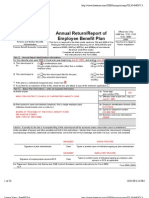
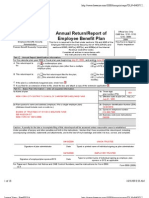
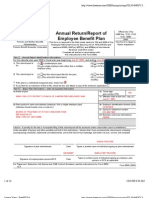
- Form 5500 Annual Return/Report of Employee Benefit Plan: X X X X X X X X X X X XDocument12 pagesForm 5500 Annual Return/Report of Employee Benefit Plan: X X X X X X X X X X X XkmccoynycNo ratings yet
- 2006 Form 5500 Carpenter Pension PlanDocument22 pages2006 Form 5500 Carpenter Pension PlanLatisha WalkerNo ratings yet
- Carpenters Welfare Fund 2007Document18 pagesCarpenters Welfare Fund 2007Latisha WalkerNo ratings yet
- Carpenters Welfare Fund 2006Document16 pagesCarpenters Welfare Fund 2006Latisha WalkerNo ratings yet
- US Internal Revenue Service: f5500sg - 1999Document4 pagesUS Internal Revenue Service: f5500sg - 1999IRSNo ratings yet
- US Internal Revenue Service: f945 - 1998Document2 pagesUS Internal Revenue Service: f945 - 1998IRSNo ratings yet
- US Internal Revenue Service: f5500 - 1994Document6 pagesUS Internal Revenue Service: f5500 - 1994IRSNo ratings yet
- Carpenters Vacation Fund 2007Document8 pagesCarpenters Vacation Fund 2007Latisha WalkerNo ratings yet
- Carpenters Vacation Fund 2006Document14 pagesCarpenters Vacation Fund 2006Latisha WalkerNo ratings yet
- US Internal Revenue Service: f945 - 2002Document2 pagesUS Internal Revenue Service: f945 - 2002IRSNo ratings yet
- US Internal Revenue Service: f5500sc - 2003Document3 pagesUS Internal Revenue Service: f5500sc - 2003IRSNo ratings yet
- Form 5500-SF 2017: Short Form Annual Return/Report of Small Employee Benefit PlanDocument3 pagesForm 5500-SF 2017: Short Form Annual Return/Report of Small Employee Benefit PlanoaifoiweuNo ratings yet
- US Internal Revenue Service: f5500sd - 2003Document4 pagesUS Internal Revenue Service: f5500sd - 2003IRSNo ratings yet
- Union Security Trust Fund 2006Document10 pagesUnion Security Trust Fund 2006Latisha WalkerNo ratings yet
- NRA 2016 401 (K) - Form 5500Document15 pagesNRA 2016 401 (K) - Form 5500jpeppardNo ratings yet
- NRA 2015 Defined Benefit Plan 5500Document19 pagesNRA 2015 Defined Benefit Plan 5500jpeppardNo ratings yet
- US Internal Revenue Service: f5500cr - 1997Document6 pagesUS Internal Revenue Service: f5500cr - 1997IRSNo ratings yet
- US Internal Revenue Service: f5500 - 1996Document6 pagesUS Internal Revenue Service: f5500 - 1996IRSNo ratings yet
- US Internal Revenue Service: f5500sc - 1998Document3 pagesUS Internal Revenue Service: f5500sc - 1998IRSNo ratings yet
- Pension PlanDocument49 pagesPension PlanPriscilla TranNo ratings yet
- US Internal Revenue Service: f5500cr - 1995Document6 pagesUS Internal Revenue Service: f5500cr - 1995IRSNo ratings yet
- US Internal Revenue Service: f5500 - 1991Document6 pagesUS Internal Revenue Service: f5500 - 1991IRSNo ratings yet
- Penn State Right-To-Know Report 2011Document66 pagesPenn State Right-To-Know Report 2011veblenNo ratings yet
- Aircraft Rental & Leasing Revenues World Summary: Market Values & Financials by CountryFrom EverandAircraft Rental & Leasing Revenues World Summary: Market Values & Financials by CountryNo ratings yet
- US Internal Revenue Service: 2290rulesty2007v4 0Document6 pagesUS Internal Revenue Service: 2290rulesty2007v4 0IRSNo ratings yet
- 2008 Objectives Report To Congress v2Document153 pages2008 Objectives Report To Congress v2IRSNo ratings yet
- 2008 Data DictionaryDocument260 pages2008 Data DictionaryIRSNo ratings yet
- 2008 Credit Card Bulk Provider RequirementsDocument112 pages2008 Credit Card Bulk Provider RequirementsIRSNo ratings yet
- 25 Data Response QuestionsDocument27 pages25 Data Response QuestionsAiza AyazNo ratings yet
- E Index 1990-2006Document519 pagesE Index 1990-2006Citra Dewi WulansariNo ratings yet
- FATCA W9 + Carta para Compartir Información (FATCA)Document2 pagesFATCA W9 + Carta para Compartir Información (FATCA)CarrilloyLawNo ratings yet
- Employee Payslip NewDocument1 pageEmployee Payslip NewRitika SharmaNo ratings yet
- Uestion Paper IftDocument48 pagesUestion Paper IftArchitAgrawalNo ratings yet
- Premium Tax Credit PTCDocument2 pagesPremium Tax Credit PTCpqr1No ratings yet
- US Internal Revenue Service: I2555ez - 2002Document3 pagesUS Internal Revenue Service: I2555ez - 2002IRSNo ratings yet
- CD TalDocument188 pagesCD Talmst04012002No ratings yet
- Income Tax Limits Days Summay by CA Vivek Gaba TAX LOVE. 1Document82 pagesIncome Tax Limits Days Summay by CA Vivek Gaba TAX LOVE. 1KrishnaNo ratings yet
- Thanksgiving Travel Forecast ReportDocument2 pagesThanksgiving Travel Forecast ReportTatiana RokouNo ratings yet
- TPoints Fee AirMilesDocument1 pageTPoints Fee AirMilesDolphin LipNo ratings yet
- The United States in The World EconomyDocument12 pagesThe United States in The World EconomyAbdul WahidNo ratings yet
- New Rekening Koran Online 493501004332535 2023-02-01 2023-02-28 00326282 PDFDocument2 pagesNew Rekening Koran Online 493501004332535 2023-02-01 2023-02-28 00326282 PDFSupebriasa AmdNo ratings yet
- MXWD As of Jun 28 20221Document124 pagesMXWD As of Jun 28 20221Wei Xiang TanNo ratings yet
- Erie County Property Transfers - December 2006Document10 pagesErie County Property Transfers - December 2006api-3705969No ratings yet
- LLC MemoDocument2 pagesLLC Memoapi-299644289No ratings yet
- Horizontal AnalysisDocument1 pageHorizontal AnalysisMahmood KhanNo ratings yet
- 1 15 2022.PayStubSJ99Document1 page1 15 2022.PayStubSJ99troymc101No ratings yet
- Oregon Tax 40Document32 pagesOregon Tax 40Nat BrewNo ratings yet
- Us Stocks DecDocument138 pagesUs Stocks DecRambhakt HanumanNo ratings yet
- OutputDocument19 pagesOutputJohnson WilliamNo ratings yet