You might also like
- IV FluidsDocument47 pagesIV FluidsMuvenn Kannan100% (1)
- 0 BOSH FrameworkDocument18 pages0 BOSH Frameworkharold fontiveros100% (1)
- Colloids and CrystalooidsDocument42 pagesColloids and Crystalooidsلؤي زعيترNo ratings yet
- Management of diabetic ketoacidosis: principles of management in the first hourDocument13 pagesManagement of diabetic ketoacidosis: principles of management in the first hourAzim Abd RazakNo ratings yet
- Electrolyte DisordersDocument10 pagesElectrolyte DisordersSlavicaNo ratings yet
- Hemorrhagic Cerebro Vascular DiseaseDocument37 pagesHemorrhagic Cerebro Vascular Diseasejbvaldez100% (1)
- Soil Loss EstimationDocument77 pagesSoil Loss Estimationmys85No ratings yet
- Infants and ToddlersDocument14 pagesInfants and ToddlersJosias Smith100% (1)
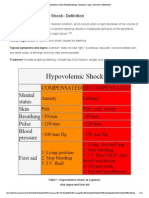
- Hypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarDocument15 pagesHypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarKaloy KamaoNo ratings yet
- Surgical Treatment For BREAST CANCERDocument5 pagesSurgical Treatment For BREAST CANCERJericho James TopacioNo ratings yet
- Heart Failure COncept MapDocument2 pagesHeart Failure COncept MapJrBong SemaneroNo ratings yet
- Anemia of Chronic Disease - Inflammation - UpToDateDocument36 pagesAnemia of Chronic Disease - Inflammation - UpToDateDomenica MurilloNo ratings yet
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Stroke and Cerebrovascular DiseaseDocument14 pagesStroke and Cerebrovascular DiseaseMarwan M.No ratings yet
- Hypovolemic ShockDocument2 pagesHypovolemic Shockatilano_patrickNo ratings yet
- Acute Renal Failure TeoriDocument24 pagesAcute Renal Failure TeoriVera Andri YaniNo ratings yet
- Acute Lymphoblastic LeukemiaDocument34 pagesAcute Lymphoblastic LeukemiamtyboyNo ratings yet
- Medscape Hypovolemic ShockDocument14 pagesMedscape Hypovolemic ShockSarah Ovinitha100% (1)
- Primary AldosteronismDocument31 pagesPrimary AldosteronismSteph100% (1)
- NSG 117 PerfusionDocument55 pagesNSG 117 PerfusionAnonymous UJEyEsNo ratings yet
- Iveco F4ge PDFDocument142 pagesIveco F4ge PDFHandy Lee67% (3)
- Early and Late Signs of Increased Intracranial PressureDocument8 pagesEarly and Late Signs of Increased Intracranial PressureRhae Raynog100% (2)
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Disorders of Hemoglobin Structure and ThalassemiasDocument10 pagesDisorders of Hemoglobin Structure and ThalassemiasManisanthosh KumarNo ratings yet
- Respiratory Medicine 1 50Document33 pagesRespiratory Medicine 1 50Ahmed Kh. Abu WardaNo ratings yet
- Diabetic KetoacidosisDocument41 pagesDiabetic KetoacidosisdenekeNo ratings yet
- CKD Complications: Improving Global ManagementDocument32 pagesCKD Complications: Improving Global ManagementmetaNo ratings yet
- Drugs Affecting Calcium BalanceDocument63 pagesDrugs Affecting Calcium BalanceRd Chandane100% (1)
- Amniotic Fluid Embolism Clinical Presentation ReviewDocument29 pagesAmniotic Fluid Embolism Clinical Presentation ReviewArun Kumar Gupta100% (1)
- Generic Name Therapeutic Classification Pharmacologic ClassificationDocument3 pagesGeneric Name Therapeutic Classification Pharmacologic ClassificationAnselle CasilNo ratings yet
- MyocarditisDocument29 pagesMyocarditispanvilai0% (1)
- 2 Acute Myocardial InfarctionDocument15 pages2 Acute Myocardial InfarctionpauchanmnlNo ratings yet
- Acute Glomerulonephritis Case StudyDocument6 pagesAcute Glomerulonephritis Case StudyjakerzNo ratings yet
- GI Diagnostic TestsDocument7 pagesGI Diagnostic TestspatzieNo ratings yet
- HYPOKALEMIA) ReportDocument72 pagesHYPOKALEMIA) ReportFairoz Macud AdapNo ratings yet
- Predisposing Conditions, Management and Prevention of Chronic Kidney DiseaseDocument52 pagesPredisposing Conditions, Management and Prevention of Chronic Kidney DiseaseSaad MotawéaNo ratings yet
- Acute Renal Failure Pathophysiology, Stages, Complications & ManagementDocument18 pagesAcute Renal Failure Pathophysiology, Stages, Complications & ManagementSteven Paul DaclesNo ratings yet
- Concise overview of chronic kidney disease (CKDDocument35 pagesConcise overview of chronic kidney disease (CKDgailNo ratings yet
- Acute Kidney InjuryDocument43 pagesAcute Kidney InjuryIwan ToniroNo ratings yet
- Types of Leukemia ExplainedDocument4 pagesTypes of Leukemia ExplainedwizardebmNo ratings yet
- Case Study: Congestive Heart FailureDocument7 pagesCase Study: Congestive Heart FailureXI-E / 21 / MARY TRIANANo ratings yet
- Hyperosmolar Hyperglycemic State (HHS)Document21 pagesHyperosmolar Hyperglycemic State (HHS)Malueth AnguiNo ratings yet
- PHARMACOLOGY - Midterms 1.6-Fluid and Electrolyte TRANSDocument13 pagesPHARMACOLOGY - Midterms 1.6-Fluid and Electrolyte TRANSNooneNo ratings yet
- Heart Failure With Preserved Ejection FractionDocument19 pagesHeart Failure With Preserved Ejection Fractioncosmin balanNo ratings yet
- Glomerulonephritis vs GlomerulopathiesDocument58 pagesGlomerulonephritis vs GlomerulopathiesRahmailla Khanza Diana FebriliantriNo ratings yet
- HyponatremiaDocument46 pagesHyponatremiaxplaindNo ratings yet
- Causes, Symptoms and Treatment of AtelectasisDocument4 pagesCauses, Symptoms and Treatment of AtelectasisAshley Jane MacapayadNo ratings yet
- Renal Failure and Kidney DiseaseDocument41 pagesRenal Failure and Kidney Disease12046No ratings yet
- NCM 106 - Case Analysis - Nursing Care Plan of Heart FailureDocument2 pagesNCM 106 - Case Analysis - Nursing Care Plan of Heart FailureMarisol Jane JomayaNo ratings yet
- Group 5 - Hemodialysis - Chronic Kidney FailureDocument31 pagesGroup 5 - Hemodialysis - Chronic Kidney FailureKimberly Abella CabreraNo ratings yet
- Uremic EncephalophatyDocument48 pagesUremic EncephalophatySindi LadayaNo ratings yet
- Hypoxia and Oxygen TherapyDocument19 pagesHypoxia and Oxygen Therapynirilib86% (7)
- Peritonitis in PD PatientsDocument64 pagesPeritonitis in PD PatientsDaniel SitungkirNo ratings yet
- Shock &) Plasma Expanders, MBBS 2012Document33 pagesShock &) Plasma Expanders, MBBS 2012Dr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- Renal Replacement TherapyDocument23 pagesRenal Replacement TherapyShelly Dwi SilvitaNo ratings yet
- Septic Shock: Supervisor: DR Ali Haedar, Sp. EM FAHA Dinisa Novaurahmah Nanin Aprilia PutriDocument42 pagesSeptic Shock: Supervisor: DR Ali Haedar, Sp. EM FAHA Dinisa Novaurahmah Nanin Aprilia PutriMutia Larasati AlbarNo ratings yet
- Cardiovascular Disease in CKD - FINAL DRAFT (26 May 2010)Document34 pagesCardiovascular Disease in CKD - FINAL DRAFT (26 May 2010)Dee DNo ratings yet
- HyponatremiaDocument44 pagesHyponatremiaALi TaLib ShukurNo ratings yet
- Organophosphrous PoisoningDocument53 pagesOrganophosphrous Poisoningpriyashu78100% (1)
- Chapter 067 Sirs ModsDocument25 pagesChapter 067 Sirs Modsapi-232466940No ratings yet
- Diagnosis and Management of Electrolyte EmergenciesDocument29 pagesDiagnosis and Management of Electrolyte EmergenciesFatin Farhana JubaidiNo ratings yet
- Phosphate Imbalances PDFDocument1 pagePhosphate Imbalances PDFKaye RicoNo ratings yet
- InhalDocument33 pagesInhallupeNo ratings yet
- Health Assessment 16Document11 pagesHealth Assessment 16shannon c. lewisNo ratings yet
- Humiseal Thinner 73 MSDSDocument3 pagesHumiseal Thinner 73 MSDSibnu Groho Herry sampurnoNo ratings yet
- Hydrogen DryerDocument2 pagesHydrogen Dryersanju_cgh5518No ratings yet
- Practical Laser Diodes GuideDocument4 pagesPractical Laser Diodes GuideM Xubair Yousaf XaiNo ratings yet
- 29 TM5 Kireina Akhlak AnnisaDocument30 pages29 TM5 Kireina Akhlak AnnisaTamaraNo ratings yet
- Adapted Sports & Recreation 2015: The FCPS Parent Resource CenterDocument31 pagesAdapted Sports & Recreation 2015: The FCPS Parent Resource CenterkirthanasriNo ratings yet
- Cognitive Development of Infants and ToddlersDocument1 pageCognitive Development of Infants and ToddlersCyrell Rondina100% (2)
- Deck Damage and Penetrations: Prepared by Richard B. Heagler, P.EDocument9 pagesDeck Damage and Penetrations: Prepared by Richard B. Heagler, P.ENelzon MamaniNo ratings yet
- Non-Directive Counselling RogersDocument5 pagesNon-Directive Counselling RogersSanjeev ChaudharyNo ratings yet
- Entrenamiento de Fuerza y Salud Pediátrica Ingles PDFDocument9 pagesEntrenamiento de Fuerza y Salud Pediátrica Ingles PDFGiiovanny PardoNo ratings yet
- Lembar Latihan - P1 - PD MitraDocument123 pagesLembar Latihan - P1 - PD MitratiengcityNo ratings yet
- Bemidji Police Department 1-14-13Document19 pagesBemidji Police Department 1-14-13John HagemanNo ratings yet
- Chloe Kho - Assignment 5 - MTT PracticeDocument5 pagesChloe Kho - Assignment 5 - MTT PracticeanthonyNo ratings yet
- Confined Space Planning ChecklistDocument3 pagesConfined Space Planning ChecklistKB100% (1)
- SKY BUILDER SILICON CITY QuotationDocument10 pagesSKY BUILDER SILICON CITY QuotationVikram SolankiNo ratings yet
- RC14001® & RCMS®: Your Guide To Implementing A Responsible Care® Management SystemDocument4 pagesRC14001® & RCMS®: Your Guide To Implementing A Responsible Care® Management SystemMohammed MehranNo ratings yet
- Review of LitetaureDocument8 pagesReview of LitetaureeswariNo ratings yet
- Research On Motivation TheoriesDocument15 pagesResearch On Motivation TheoriesNayeem Md SakibNo ratings yet
- Caffeine's Effect on Daphnia Heart RateDocument2 pagesCaffeine's Effect on Daphnia Heart RateMianto NamikazeNo ratings yet
- Grade 6 School Lesson on Propagating Trees and Fruit TreesDocument10 pagesGrade 6 School Lesson on Propagating Trees and Fruit TreesGhrazy Ganabol LeonardoNo ratings yet
- Face Port Port Retainer Nose Block HiDocument7 pagesFace Port Port Retainer Nose Block HiOzan EgemenNo ratings yet
- Quality and Functionality of Excipients-Art (Alumnos-S) PDFDocument14 pagesQuality and Functionality of Excipients-Art (Alumnos-S) PDFLaura PerezNo ratings yet
- NECC Sri Lanka May 2017 An Open Appeal To UN and International Community PDFDocument18 pagesNECC Sri Lanka May 2017 An Open Appeal To UN and International Community PDFThavam RatnaNo ratings yet
- D 2144 - 01 - RdixndqDocument4 pagesD 2144 - 01 - RdixndqjayakumarNo ratings yet
- Carbon Steel Alloys Steel, Pipe Dimension With Weight Test Pressures According To ANSI B36, 10 For ASTM A53/A 106/API 5L/A335/ SpecificationDocument6 pagesCarbon Steel Alloys Steel, Pipe Dimension With Weight Test Pressures According To ANSI B36, 10 For ASTM A53/A 106/API 5L/A335/ SpecificationsanjibkrjanaNo ratings yet
- Mini-Pitch Session Exceptionalities and InclusionDocument18 pagesMini-Pitch Session Exceptionalities and Inclusionapi-486583325No ratings yet