You might also like
- Word Association PANCEDocument31 pagesWord Association PANCEnevmerka100% (1)
- Medicine Cheat SheetsDocument16 pagesMedicine Cheat SheetsRisa Muthmainah100% (1)
- Clinical MedicineDocument18 pagesClinical MedicineRishikesh AsthanaNo ratings yet
- Urinary Tract InfectionDocument9 pagesUrinary Tract InfectionTom Mallinson100% (1)
- Load ScheduleDocument8 pagesLoad SchedulemerebookNo ratings yet
- PericarditisDocument29 pagesPericarditisPavin KumarNo ratings yet
- Cardiovascular Dysfunction: (Patent Ductus Arteriosus)Document6 pagesCardiovascular Dysfunction: (Patent Ductus Arteriosus)Jc MacujaNo ratings yet
- Differential Diagnosis For : DDX For in AIDS PatientsDocument32 pagesDifferential Diagnosis For : DDX For in AIDS PatientsSom Lakhani100% (2)
- ECGInterpretation Cheat SheetDocument1 pageECGInterpretation Cheat SheetTom Mallinson100% (1)
- Neurological Examination: ObserveDocument9 pagesNeurological Examination: ObserveTom MallinsonNo ratings yet
- MCQ 1. Heart Sound Heart Sound S1 S2Document7 pagesMCQ 1. Heart Sound Heart Sound S1 S2Atirah AaNo ratings yet
- Presenting Symptoms:: Gastrointestinal HistoryDocument4 pagesPresenting Symptoms:: Gastrointestinal HistoryTom MallinsonNo ratings yet
- Clinical Medicine Cheat Sheet Ebook PDFDocument18 pagesClinical Medicine Cheat Sheet Ebook PDFMokaNo ratings yet
- Ilmu KhotifDocument28 pagesIlmu KhotifAndré Martins78% (27)
- Deep Vein Thrombosis: Dr. Iman Haryana SPJPDocument29 pagesDeep Vein Thrombosis: Dr. Iman Haryana SPJPAuliyah SeptianiNo ratings yet
- Migraine Migraine Migraine Migraine: History of Presenting IllnessDocument22 pagesMigraine Migraine Migraine Migraine: History of Presenting IllnessTom MallinsonNo ratings yet
- Congenital Heart DefectsDocument7 pagesCongenital Heart DefectsJulia Rae Delos SantosNo ratings yet
- Congenital Heart DiseaseDocument8 pagesCongenital Heart DiseaseSanthosh.S.U100% (3)
- Spinal Cord InjuryDocument17 pagesSpinal Cord InjuryTom MallinsonNo ratings yet
- Shadow UAV HandbookDocument57 pagesShadow UAV HandbookGasMaskBob100% (2)
- PANCE Word Associations PDFDocument27 pagesPANCE Word Associations PDFkatNo ratings yet
- Chest Pain Investigation Diagnosis and TreatmentDocument4 pagesChest Pain Investigation Diagnosis and TreatmentHadsabsaNo ratings yet
- Traditional EmbroideryDocument38 pagesTraditional EmbroiderySabrina SuptiNo ratings yet
- Materi 12 IMELS - Trombosis Emboli Paru, Iskemik Tungkai Akut - KritisDocument64 pagesMateri 12 IMELS - Trombosis Emboli Paru, Iskemik Tungkai Akut - KritismaharyadyNo ratings yet
- Alarm Symptoms of Hematoonco in Pediatrics: Dr. Cece Alfalah, M.Biomed, Sp.A (K) Pediatric Hematology and OncologyDocument22 pagesAlarm Symptoms of Hematoonco in Pediatrics: Dr. Cece Alfalah, M.Biomed, Sp.A (K) Pediatric Hematology and OncologyMuhammad ArifNo ratings yet
- P EmbolismDocument29 pagesP EmbolismCommandoCitotz100% (1)
- Steam Purity Considerations For New TurbinesDocument46 pagesSteam Purity Considerations For New Turbinesomertrik100% (1)
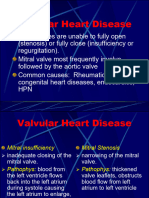
- Valvular Heart DiseaseDocument8 pagesValvular Heart DiseaseHASNIZZAM BIN AHMAD AMIN -No ratings yet
- Lump GeneralDocument5 pagesLump GeneralMoh MutawaNo ratings yet
- Mitral StenosisDocument2 pagesMitral StenosisitsmailbbkNo ratings yet
- Chronic Limb Ischemia: Prof. Dr. A.B.Singh UnitDocument59 pagesChronic Limb Ischemia: Prof. Dr. A.B.Singh UnitDr. Saad SiddiquiNo ratings yet
- Arterial Hypertension Eng PDFDocument29 pagesArterial Hypertension Eng PDFagustinaw1981No ratings yet
- Edematous SyndromeDocument4 pagesEdematous SyndromemyverseletsNo ratings yet
- Deep Vein ThrombisisDocument13 pagesDeep Vein ThrombisisDex RayNo ratings yet
- Cardiovascular Pathology: Hypertensive RetinopathyDocument7 pagesCardiovascular Pathology: Hypertensive RetinopathyTom TsouNo ratings yet
- Leptospirosis: A. Leptospiremic Phase B. Immune Phase C. Convalescent PhaseDocument3 pagesLeptospirosis: A. Leptospiremic Phase B. Immune Phase C. Convalescent PhaseAmalia PutriNo ratings yet
- Cardiovascular Shoutouts: When She Says You SayDocument7 pagesCardiovascular Shoutouts: When She Says You SayGbotemi AlaladeNo ratings yet
- Anak 2Document107 pagesAnak 2Nency PurmayaNo ratings yet
- ACC Jimmy AsafDocument152 pagesACC Jimmy AsafFikriYTNo ratings yet
- HIS1-K36 VTE, Diagnosis Klinis DVTDocument26 pagesHIS1-K36 VTE, Diagnosis Klinis DVTPaul Behring ManurungNo ratings yet
- Cardiovascular Disorders in Children - StudentDocument53 pagesCardiovascular Disorders in Children - StudentKeanu Win CatipayNo ratings yet
- Professor Rajibul Alam Sir Ward NoteDocument12 pagesProfessor Rajibul Alam Sir Ward NoteRoll-30 Um-12 Sifat DewanNo ratings yet
- Cardio Day 3 TemplateDocument24 pagesCardio Day 3 TemplateMikeNo ratings yet
- Chest Pain - Investigation, Diagnosis and TreatmentDocument5 pagesChest Pain - Investigation, Diagnosis and Treatmentsoumabho paruiNo ratings yet
- Drug Study For Nsy DRDocument4 pagesDrug Study For Nsy DRLiza M. PurocNo ratings yet
- Infectious Diseases of The HeartDocument2 pagesInfectious Diseases of The HeartJulia Rae Delos SantosNo ratings yet
- 2.4. Vena LimfeDocument28 pages2.4. Vena Limfeira citraNo ratings yet
- Dr. Witra Irfan, SP.B (K) V - DVTDocument29 pagesDr. Witra Irfan, SP.B (K) V - DVTmuhammad azharanNo ratings yet
- Notes SC CVSDocument6 pagesNotes SC CVS202213No ratings yet
- Talley Sum Up ExaminationDocument57 pagesTalley Sum Up ExaminationGroup 14No ratings yet
- Coronary Artery DiseaseDocument3 pagesCoronary Artery DiseaseRitz CelsoNo ratings yet
- (Type The Documen T Title) : Jeffrey ConnorDocument50 pages(Type The Documen T Title) : Jeffrey ConnorJeffrey HingNo ratings yet
- Onset Sign and SymptomsDocument1 pageOnset Sign and SymptomsselenaNo ratings yet
- Clinical AutopsyDocument2 pagesClinical Autopsyapi-352560644No ratings yet
- VHD To DVTDocument55 pagesVHD To DVTShiehan Mae ForroNo ratings yet
- Cardiovascular ExaminationDocument10 pagesCardiovascular ExaminationSaurabh PaudyalNo ratings yet
- Appendix 4: Common Short Cases: Cardiology RheumatologyDocument1 pageAppendix 4: Common Short Cases: Cardiology RheumatologySKNo ratings yet
- DISEASES Kawasaki, RHD, Is HPN)Document9 pagesDISEASES Kawasaki, RHD, Is HPN)jenn212No ratings yet
- Perivascular DiseasesDocument5 pagesPerivascular DiseasesKathleen Ellize BetchaydaNo ratings yet
- JVP Measured at 3 CM Above The Sternal Angle, or 8 CM Above The Right Atrium, Is Considered Elevated or AbnormalDocument11 pagesJVP Measured at 3 CM Above The Sternal Angle, or 8 CM Above The Right Atrium, Is Considered Elevated or AbnormalRubie Ann TillorNo ratings yet
- Polycystic Kidneys: Adult PKD: ComplicationsDocument1 pagePolycystic Kidneys: Adult PKD: ComplicationsUsman Ali AkbarNo ratings yet
- List of Medical Triads, Tetrads, and PentadsDocument5 pagesList of Medical Triads, Tetrads, and PentadsHajer BassemNo ratings yet
- Chest PainDocument18 pagesChest PainRajamanickam DilshanthNo ratings yet
- Case Report: Phlegmasia Cerulea Dolens: Case Report On A HIV-AIDS Patient in A Sub-Saharian Semi-Urban PracticeDocument5 pagesCase Report: Phlegmasia Cerulea Dolens: Case Report On A HIV-AIDS Patient in A Sub-Saharian Semi-Urban PracticeUmmi KaltsumNo ratings yet
- 14.1. Chest Pain-朱悫Document108 pages14.1. Chest Pain-朱悫mirabel IvanaliNo ratings yet
- ch28 Notes Part 2Document9 pagesch28 Notes Part 2Monica JubaneNo ratings yet
- Sindromatologi DyspneuDocument18 pagesSindromatologi DyspneuMeylan TaebenuNo ratings yet
- Imperial CardioDocument6 pagesImperial CardioDelos Santos John Lorenz ANo ratings yet
- Diagnostic Diferential Medicina InternaDocument6 pagesDiagnostic Diferential Medicina InternaLary ArNo ratings yet
- Reflection TemplateDocument1 pageReflection TemplateTom MallinsonNo ratings yet
- New CPD TemplateDocument1 pageNew CPD TemplateTom MallinsonNo ratings yet
- Self Audit of DrugsDocument2 pagesSelf Audit of DrugsTom MallinsonNo ratings yet
- The Acute Distended AbdomenDocument2 pagesThe Acute Distended AbdomenTom Mallinson100% (1)
- Self Audit of CallsDocument2 pagesSelf Audit of CallsTom MallinsonNo ratings yet
- Critical Incident TemplateDocument2 pagesCritical Incident TemplateTom MallinsonNo ratings yet
- Pulmonary Thrombo EmbolismDocument3 pagesPulmonary Thrombo EmbolismTom MallinsonNo ratings yet
- Vertebral Artery DissectionDocument2 pagesVertebral Artery DissectionTom MallinsonNo ratings yet
- Renal History and ExamDocument6 pagesRenal History and ExamTom MallinsonNo ratings yet
- Preoperative AssessmentDocument2 pagesPreoperative AssessmentTom MallinsonNo ratings yet
- Speech ExamDocument2 pagesSpeech ExamTom MallinsonNo ratings yet
- Syncope and PalpitationsDocument1 pageSyncope and PalpitationsTom MallinsonNo ratings yet
- Procedures and Explanations of ProceduresDocument13 pagesProcedures and Explanations of ProceduresTom MallinsonNo ratings yet
- Pediatric History BrieflyDocument4 pagesPediatric History BrieflyTom MallinsonNo ratings yet
- Paracetamol OverdoseDocument2 pagesParacetamol OverdoseTom MallinsonNo ratings yet
- Post Op AnalgesiaDocument2 pagesPost Op AnalgesiaTom MallinsonNo ratings yet
- NEUROHISTORYDocument2 pagesNEUROHISTORYTom MallinsonNo ratings yet
- Perioperative Pain ManagementDocument1 pagePerioperative Pain ManagementTom MallinsonNo ratings yet
- Hypersensitivity Reaction TypesDocument1 pageHypersensitivity Reaction TypesTom MallinsonNo ratings yet
- Ear, Nose & Throat - Pneumonia and Otitis MediaDocument14 pagesEar, Nose & Throat - Pneumonia and Otitis Media20094113No ratings yet
- Fractures and Compartment SyndromeDocument4 pagesFractures and Compartment SyndromeTom MallinsonNo ratings yet
- HeadacheDocument1 pageHeadacheTom MallinsonNo ratings yet
- Look:: Gastrointestinal ExamDocument6 pagesLook:: Gastrointestinal ExamTom MallinsonNo ratings yet
- Musculoskeletal History: Basic InfoDocument10 pagesMusculoskeletal History: Basic InfoTom MallinsonNo ratings yet
- 1 Soundcraft Notepad User GuideDocument40 pages1 Soundcraft Notepad User GuideNives KurjakNo ratings yet
- DST Tmpm370fydfg-Tde en 21751Document498 pagesDST Tmpm370fydfg-Tde en 21751trân văn tuấnNo ratings yet
- The Coffee Shop Easy Reading - 152542Document1 pageThe Coffee Shop Easy Reading - 152542Fc MakmurNo ratings yet
- Alternatives To Shifting Cultivation-248Document9 pagesAlternatives To Shifting Cultivation-248Chandrashekhar KhobragadeNo ratings yet
- Inguinal Hernia - QuizDocument17 pagesInguinal Hernia - Quizemily5890No ratings yet
- Parts PrecedentDocument252 pagesParts PrecedentOscar PinzonNo ratings yet
- ECE 374 - Part - 1c - S2017Document37 pagesECE 374 - Part - 1c - S2017Zakaria ElwalilyNo ratings yet
- Core12 Mod 1Document1 pageCore12 Mod 1Michael SaberonNo ratings yet
- Chapter 13 Managerial AccountingDocument168 pagesChapter 13 Managerial AccountingChandler Schleifs100% (4)
- Regulatory Framework For Water Dams in QuebecDocument2 pagesRegulatory Framework For Water Dams in QuebecRaveeNo ratings yet
- Pastor O. I. Kirk, SR D.D LIFE Celebration BookDocument63 pagesPastor O. I. Kirk, SR D.D LIFE Celebration Booklindakirk1100% (1)
- Transportation ProblemDocument4 pagesTransportation ProblemPrejit RadhakrishnaNo ratings yet
- Origami Undergrad ThesisDocument63 pagesOrigami Undergrad ThesisEduardo MullerNo ratings yet
- BHS Inggris 2021Document6 pagesBHS Inggris 2021Muhammad FirmanNo ratings yet
- TamasDocument180 pagesTamaslike 2No ratings yet
- Curriculum Jaime Alvarado (Jaime Alvarado)Document3 pagesCurriculum Jaime Alvarado (Jaime Alvarado)yuly aldanaNo ratings yet
- Mits Chocolates: Let The Life Be More Sweet'Document30 pagesMits Chocolates: Let The Life Be More Sweet'Azaz NathaniNo ratings yet
- 5 - Oral Mucosa and Salivary Glands (Mahmoud Bakr)Document115 pages5 - Oral Mucosa and Salivary Glands (Mahmoud Bakr)MobarobberNo ratings yet
- Stahl - PUDSDocument29 pagesStahl - PUDSsusanasusana_No ratings yet
- History of Costa RicaDocument2 pagesHistory of Costa Ricakrishnan MishraNo ratings yet
- Ansi/Isa - 75.08.04-2001 (R2013) Face-to-Face Dimensions For Buttweld-End Globe-Style Control Valves (Class 4500)Document16 pagesAnsi/Isa - 75.08.04-2001 (R2013) Face-to-Face Dimensions For Buttweld-End Globe-Style Control Valves (Class 4500)Horas CanmanNo ratings yet
- Mohd Mopti Bin Yassin V Lembaga Kemajuan Perusahaan Pertanian Negeri Pahang (LKPP) Corp SDN BHD & AnorDocument12 pagesMohd Mopti Bin Yassin V Lembaga Kemajuan Perusahaan Pertanian Negeri Pahang (LKPP) Corp SDN BHD & AnorA random humanNo ratings yet
- Danh M C AHTN 2017 - HS Code 2017 PDFDocument564 pagesDanh M C AHTN 2017 - HS Code 2017 PDFBao Ngoc Nguyen100% (1)
- Dense NetDocument28 pagesDense NetFahad RazaNo ratings yet
- Dynamic-Light-Scattering - MDLDocument5 pagesDynamic-Light-Scattering - MDLJose Daniel Izquierdo MorenoNo ratings yet