You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Certifying Statement Application Results and Certificates Form 7Document4 pagesCertifying Statement Application Results and Certificates Form 7Haider QureshiNo ratings yet
- NIL Case Digests - Dec. 1, 2018 Assigned ReadingDocument13 pagesNIL Case Digests - Dec. 1, 2018 Assigned ReadingMarianne Hope VillasNo ratings yet
- Québec CAQ Application GuideDocument4 pagesQuébec CAQ Application GuideSM MANAGEMENTNo ratings yet
- Psychology Provisional Registration ApplicationDocument12 pagesPsychology Provisional Registration ApplicationcristimocanitaNo ratings yet
- Types of non-negotiable financial instrumentsDocument15 pagesTypes of non-negotiable financial instrumentsSenthil MassenNo ratings yet
- T 5Document10 pagesT 5api-443605501No ratings yet
- Authorisation LetterDocument2 pagesAuthorisation Letterpraviknr67% (6)
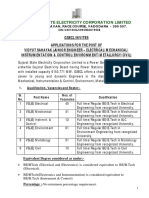
- GSECL Recruitment for 100+ VacanciesDocument8 pagesGSECL Recruitment for 100+ VacanciesVikasMantriNo ratings yet
- Neil Wallace Paper Sale November PDFDocument8 pagesNeil Wallace Paper Sale November PDFARTroom2012No ratings yet
- Application For Official SearchDocument2 pagesApplication For Official SearchDavis kipronoNo ratings yet
- PF Withdrawal Application (Sample Copy)Document5 pagesPF Withdrawal Application (Sample Copy)Ravi Kant Thakur80% (5)
- Registration Procedure for Inspector of Works MalaysiaDocument3 pagesRegistration Procedure for Inspector of Works MalaysiaAmirah IdrusNo ratings yet
- Sunshine Challenge AnnouncementDocument3 pagesSunshine Challenge Announcementapi-241437399No ratings yet
- Delhi Metro Rail Job OpeningsDocument8 pagesDelhi Metro Rail Job OpeningsRamanuja SuriNo ratings yet
- Moneygram Receipt Reference Number TrackingDocument19 pagesMoneygram Receipt Reference Number TrackingFonfo Lawrence0% (1)
- Visa ScreenDocument29 pagesVisa ScreenpytotNo ratings yet
- Foreign Exchange of Jamuna Bank Ltd.Document56 pagesForeign Exchange of Jamuna Bank Ltd.arifNo ratings yet
- Membership & Payment FormDocument3 pagesMembership & Payment FormAtharva KannavNo ratings yet
- Managment Project of Habib BankDocument32 pagesManagment Project of Habib BankAamir Raza50% (2)
- Internship Report RimshaDocument24 pagesInternship Report RimshaRimsha ButtNo ratings yet
- 11076EDocument0 pages11076EDilpreet SinghNo ratings yet
- SSS Employer Contributions FormDocument2 pagesSSS Employer Contributions FormUncle Cheffy - MalateNo ratings yet
- Philippine Education Co vs Soriano Dispute Over Stolen Postal Money OrderDocument4 pagesPhilippine Education Co vs Soriano Dispute Over Stolen Postal Money OrderKeej DalonosNo ratings yet
- Promissory Note Vs Bill PF ExchangeDocument2 pagesPromissory Note Vs Bill PF ExchangelexscribisNo ratings yet
- Philippine Education Co v. Mauricio Soriano, Et Al.Document2 pagesPhilippine Education Co v. Mauricio Soriano, Et Al.Katrina PerezNo ratings yet
- Internship Report ON "Foreign Exchange System of Rupali Bank Limited"Document37 pagesInternship Report ON "Foreign Exchange System of Rupali Bank Limited"Shakhauat HossainNo ratings yet
- Contractor Licence Application Natural PersonDocument12 pagesContractor Licence Application Natural PersonApollo ApollpNo ratings yet
- Accounting For Government Revenue in TanzaniaDocument9 pagesAccounting For Government Revenue in TanzaniaChristopher John MwakipesileNo ratings yet
- Admission FormDocument2 pagesAdmission Formjlast23No ratings yet
- Application for Gratuity PaymentDocument6 pagesApplication for Gratuity PaymentDigraj MahantaNo ratings yet