You might also like
- The Physiologic Effects of Neuraxial BlocksDocument5 pagesThe Physiologic Effects of Neuraxial BlocksSuresh KumarNo ratings yet
- Cardiovascular Effects of PropofolDocument6 pagesCardiovascular Effects of PropofoluzmaNo ratings yet
- 127 WilliamsDocument9 pages127 WilliamsRikizu HobbiesNo ratings yet
- Review ArticleDocument14 pagesReview ArticleBùi Ngọc Anh HSTCNo ratings yet
- JURNALDocument8 pagesJURNALICHWANUDDINBUCHORINo ratings yet
- 2020 Sanjeev Physiology International 2020Document15 pages2020 Sanjeev Physiology International 2020maloymandalNo ratings yet
- Isolated Pulmonary Regurgitation Causes Decreased Right Ventricular Longitudinal Function and Compensatory Increased Septal Pumping in A Porcine ModelDocument26 pagesIsolated Pulmonary Regurgitation Causes Decreased Right Ventricular Longitudinal Function and Compensatory Increased Septal Pumping in A Porcine ModelRAHUL KUMARNo ratings yet
- 1 s2.0 S1053249819316845 MainDocument9 pages1 s2.0 S1053249819316845 MainPatrizio SartiniNo ratings yet
- Monitoring Fluid ResponsivenessDocument7 pagesMonitoring Fluid Responsivenessvaleria SepviNo ratings yet
- CardiorespiratoryDocument10 pagesCardiorespiratoryEdi Saputra SNo ratings yet
- Optimizare Parametrii CRT Cu EcoDocument13 pagesOptimizare Parametrii CRT Cu EcoCatrinaBiancaNo ratings yet
- Cerebral Ischemia in Patients With Atrial FibrillationDocument4 pagesCerebral Ischemia in Patients With Atrial FibrillationCentral Asian StudiesNo ratings yet
- Comparative Analysis of Radiocephalic Versus Brach PDFDocument7 pagesComparative Analysis of Radiocephalic Versus Brach PDFandikeNo ratings yet
- Can Transient BP High Risk Cerebral InfarctsDocument9 pagesCan Transient BP High Risk Cerebral InfarctsshofidhiaaaNo ratings yet
- Continuous Hemodynamic MonitoringDocument54 pagesContinuous Hemodynamic MonitoringOrion JohnNo ratings yet
- Physical Exercise Reduces Transplant Arteriosclerosis in A Mouse Aorta Transplantation ModelDocument8 pagesPhysical Exercise Reduces Transplant Arteriosclerosis in A Mouse Aorta Transplantation ModelNicoleta Popa-FoteaNo ratings yet
- Revisiting The Role of Oxygen Therapy in Cardiac Patients: Raman Moradkhan, MD, Lawrence I. Sinoway, MDDocument4 pagesRevisiting The Role of Oxygen Therapy in Cardiac Patients: Raman Moradkhan, MD, Lawrence I. Sinoway, MDIda LemonNo ratings yet
- The Effect of Cilostazol On Right Heart FunctionDocument43 pagesThe Effect of Cilostazol On Right Heart FunctionGunawan YogaNo ratings yet
- Cpap Vs Vni - PasquinaDocument8 pagesCpap Vs Vni - PasquinaMelina AlcaineNo ratings yet
- VVS y VPP EN CIRUGÍA CARDÍACA BYPASS SIN CEC - 2005Document7 pagesVVS y VPP EN CIRUGÍA CARDÍACA BYPASS SIN CEC - 2005Elsa AivarNo ratings yet
- Carvedilol and Nebivolol Improve Left Ventricular Systolic Functions in Patients With Non-Ischemic Heart FailureDocument6 pagesCarvedilol and Nebivolol Improve Left Ventricular Systolic Functions in Patients With Non-Ischemic Heart FailureBramantyo DwiputraNo ratings yet
- Impact of Remote Ischaemic Preconditioning On Cerebral Oxygenation During Total Knee ArthroplastyDocument8 pagesImpact of Remote Ischaemic Preconditioning On Cerebral Oxygenation During Total Knee ArthroplastySanti ParambangNo ratings yet
- Pathophysiology of COPDDocument4 pagesPathophysiology of COPDrinieeeNo ratings yet
- Preoperative Cerebral Oxygen Saturation and Clinical Outcomes in Cardiac SurgeryDocument12 pagesPreoperative Cerebral Oxygen Saturation and Clinical Outcomes in Cardiac SurgeryThotaNo ratings yet
- Journal Homepage: - : IntroductionDocument13 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Ten Tips To Optimize VasopressorsDocument4 pagesTen Tips To Optimize VasopressorsSimon HiouNo ratings yet
- Efficacy of Hyperventilation, Blood Pressure Elevation, and Metabolic Suppression Therapy in Controlling Intracranial Pressure After Head InjuryDocument9 pagesEfficacy of Hyperventilation, Blood Pressure Elevation, and Metabolic Suppression Therapy in Controlling Intracranial Pressure After Head InjuryAik NoeraNo ratings yet
- Journal ReadingDocument17 pagesJournal ReadingRhyka AchmadNo ratings yet
- Disertasi Dr. TerawanDocument8 pagesDisertasi Dr. TerawanNurhaidah AchmadNo ratings yet
- Transcranial Doppler: An Introduction For Primary Care PhysiciansDocument7 pagesTranscranial Doppler: An Introduction For Primary Care PhysiciansdediNo ratings yet
- Tenecteplae AlteplaseDocument7 pagesTenecteplae AlteplaseHugo ARNo ratings yet
- Vti Carotideo RevisarDocument9 pagesVti Carotideo RevisarCurro MirallesNo ratings yet
- Okello2017 Article RheumaticHeartDiseaseInUgandaPDocument10 pagesOkello2017 Article RheumaticHeartDiseaseInUgandaPyosefinNo ratings yet
- Parasympathetic Overactivity in Patients With Nasal Septum DeformitiesDocument5 pagesParasympathetic Overactivity in Patients With Nasal Septum DeformitiesDwi juliana DewiNo ratings yet
- CLN 66 01 107 PDFDocument5 pagesCLN 66 01 107 PDFGloria KartikaNo ratings yet
- Fodor2019 Article OptimalCrystalloidVolumeRatioFDocument9 pagesFodor2019 Article OptimalCrystalloidVolumeRatioFIvan MoralesNo ratings yet
- Free-Diving - Control of Cerebral Blood FlowDocument5 pagesFree-Diving - Control of Cerebral Blood FlowTek StormanNo ratings yet
- Plan of Thesis VishalDocument24 pagesPlan of Thesis Vishalvishaljha86No ratings yet
- Critical Apraisal: Posisi Telungkup Secara Signifikan Mengurangi Angka Kematian Dibandingkan Dengan Posisi TelentangDocument9 pagesCritical Apraisal: Posisi Telungkup Secara Signifikan Mengurangi Angka Kematian Dibandingkan Dengan Posisi TelentangRiakan MangkaNo ratings yet
- EPITHET Failed Chance or New HopeDocument2 pagesEPITHET Failed Chance or New HopeMondo BijaineNo ratings yet
- Intensive - Care - Medicine. VasopressorDocument4 pagesIntensive - Care - Medicine. VasopressorSa7arNo ratings yet
- Treatment: Stroke UnitDocument6 pagesTreatment: Stroke Unitgraze_hinataNo ratings yet
- Indikasi Bronkoskopi: Table 3 Table 4Document5 pagesIndikasi Bronkoskopi: Table 3 Table 4Gratcia AyundiniNo ratings yet
- FALLA CARDIACA CRÒNICA y Marcadores Pronòsticos HEART 2004Document6 pagesFALLA CARDIACA CRÒNICA y Marcadores Pronòsticos HEART 2004jomalu210377No ratings yet
- Venodila Tion Contributes Hypotension in Humans To Propofol-Media TedDocument7 pagesVenodila Tion Contributes Hypotension in Humans To Propofol-Media TedArun DavesarNo ratings yet
- Cheng 2017Document6 pagesCheng 2017Lepaca KliffothNo ratings yet
- Reviews: Hyperventilation in Head InjuryDocument16 pagesReviews: Hyperventilation in Head InjurySani Widya FirnandaNo ratings yet
- Japplphysiol 00241 2022Document11 pagesJapplphysiol 00241 2022Rafael Yokoyama FecchioNo ratings yet
- Minimalist Introduction To Anesthesiology Rev 1.5Document12 pagesMinimalist Introduction To Anesthesiology Rev 1.5Syafiqah HaniNo ratings yet
- Coronary Artery Occlusions Diagnosed by Transthoracic DopplerDocument11 pagesCoronary Artery Occlusions Diagnosed by Transthoracic DopplerNag Mallesh RaoNo ratings yet
- Chan 2014Document7 pagesChan 2014denanurbaniazharNo ratings yet
- Effect of Nocturnal Oxygen Therapy On Electrocardiographic Changes Among Patients With Congestive Heart FailureDocument3 pagesEffect of Nocturnal Oxygen Therapy On Electrocardiographic Changes Among Patients With Congestive Heart FailureNurAfifahNo ratings yet
- Hemodynamic Monitoring in ShockDocument6 pagesHemodynamic Monitoring in Shockdiana25No ratings yet
- Ajpheart 00081 2017Document13 pagesAjpheart 00081 2017jorge escobar pintoNo ratings yet
- IHD Vitamin CDocument17 pagesIHD Vitamin CFarrah ErmanNo ratings yet
- Effect of Open and Closed Endotracheal Suction Systems On Heart Rhythm and Arterial Blood Oxygen Level in Intensive Care Unit PatientsDocument4 pagesEffect of Open and Closed Endotracheal Suction Systems On Heart Rhythm and Arterial Blood Oxygen Level in Intensive Care Unit PatientsNersB 11No ratings yet
- JcsmJC1900562 W22pod AnsweredDocument13 pagesJcsmJC1900562 W22pod Answeredlion5835No ratings yet
- Guinot2017 PDFDocument9 pagesGuinot2017 PDFFIA SlotNo ratings yet
- Revista Brasileira DE AnestesiologiaDocument9 pagesRevista Brasileira DE AnestesiologiayulianiNo ratings yet
- Cat Dissection FULLDocument9 pagesCat Dissection FULLPrince Nur-Hakeem BuisanNo ratings yet
- Mitral Stenosis (MS) X Mitral Regurgitasi (MR)Document25 pagesMitral Stenosis (MS) X Mitral Regurgitasi (MR)Nur Faydotus SalsabilaNo ratings yet
- Immunology of The Lymphatic System PDFDocument180 pagesImmunology of The Lymphatic System PDFCNPOULISNo ratings yet
- Endovascular Versus Surgical Revascularization For Acute Limb IschemiaDocument9 pagesEndovascular Versus Surgical Revascularization For Acute Limb IschemiaSisca Dwi AgustinaNo ratings yet
- Conduction System of The HeartDocument9 pagesConduction System of The Hearthirap0% (1)
- Asian Management of Hypertension: Current Status, Home Blood Pressure, and Specific Concerns in Philippines (A Country Report)Document4 pagesAsian Management of Hypertension: Current Status, Home Blood Pressure, and Specific Concerns in Philippines (A Country Report)DORINNE KINDAONo ratings yet
- GLENN SHUNT-Anesthetic Concerns For A Non Cardiac SurgeryDocument8 pagesGLENN SHUNT-Anesthetic Concerns For A Non Cardiac SurgeryMore InterestingNo ratings yet
- GE Voluson Ie Reference ManualDocument416 pagesGE Voluson Ie Reference Manualthaimedicaltrading THNo ratings yet
- Acute Coronary Syndrome (Myocardial Infarction and Unstable Angina) (Clinical) - LecturioDocument36 pagesAcute Coronary Syndrome (Myocardial Infarction and Unstable Angina) (Clinical) - Lecturiokujtimepira2No ratings yet
- Blood VesselsDocument13 pagesBlood VesselsAmy JessyNo ratings yet
- Mortality RateDocument5 pagesMortality RateAlquino Heart RubioNo ratings yet
- Transport in Humans: Test Yourself 8.1 (Page 140)Document3 pagesTransport in Humans: Test Yourself 8.1 (Page 140)lee100% (3)
- RomagnoliDocument8 pagesRomagnoliserena7205No ratings yet
- LITFL - Wellens SyndromeDocument8 pagesLITFL - Wellens Syndromesunil abrahamNo ratings yet
- % Chapter 3: Regulation of Gas Content in BloodDocument33 pages% Chapter 3: Regulation of Gas Content in BloodK CNo ratings yet
- Chapter 5: Analyzing A Rhythm StripDocument7 pagesChapter 5: Analyzing A Rhythm StriptellyNo ratings yet
- Han Cmu 0041E 10605Document155 pagesHan Cmu 0041E 10605Buse Nur AkçayNo ratings yet
- 001 Ara Cchi Mini Glossary Cardiovascular v2Document5 pages001 Ara Cchi Mini Glossary Cardiovascular v2Smile Al MosabyNo ratings yet
- Langley 1927Document7 pagesLangley 1927Vatsal SinghNo ratings yet
- Acute Coronary SyndromesDocument47 pagesAcute Coronary SyndromeshorosuNo ratings yet
- Cardiac Stress Testing - Choosing The Right Test and WhenDocument75 pagesCardiac Stress Testing - Choosing The Right Test and WhenLakshmi PrasannaNo ratings yet
- Carotid Artery DiseaseDocument48 pagesCarotid Artery DiseaseAdeleye John AdebolaNo ratings yet
- Science 9 1.4 Circulation of Blood in The BodyDocument13 pagesScience 9 1.4 Circulation of Blood in The BodyChad Kirsten Mier LustreNo ratings yet
- Lesson 1: Prepared By: Mark Christian N. LunaDocument28 pagesLesson 1: Prepared By: Mark Christian N. LunaJohn Mark CelosaNo ratings yet
- 036.12 - Cardiovascular Pharmacology) VasopressorsDocument14 pages036.12 - Cardiovascular Pharmacology) VasopressorsOliver JacobeNo ratings yet
- Myocardial Infarction: Ericka Jane S. Barrios, R.NDocument55 pagesMyocardial Infarction: Ericka Jane S. Barrios, R.NdantefuerteNo ratings yet
- Epidemiology Feb 23 Falcon SPMDocument1 pageEpidemiology Feb 23 Falcon SPMsquidward lmaoNo ratings yet
- Carp TrialDocument10 pagesCarp TrialIMNo ratings yet
- Medication - ALT-Template - AmlodipineDocument1 pageMedication - ALT-Template - AmlodipineNancyAmissahNo ratings yet
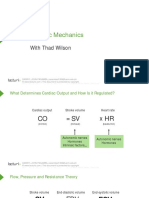
- Cardiac Mechanics: With Thad WilsonDocument26 pagesCardiac Mechanics: With Thad WilsonpasambalyrradjohndarNo ratings yet