You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Lecture 9 - Symmetry & Concentricity, Expanded Position TolerancingDocument19 pagesLecture 9 - Symmetry & Concentricity, Expanded Position Tolerancingג'ון ירוקNo ratings yet
- Belajar Bahasa Spanyol PDFDocument5 pagesBelajar Bahasa Spanyol PDFHimawan PrasojoNo ratings yet
- Breaking Into The Movies: Public Pedagogy and The Politics of FilmDocument10 pagesBreaking Into The Movies: Public Pedagogy and The Politics of FilmDouglasNo ratings yet
- Optimal Voltage RegulatorDocument8 pagesOptimal Voltage RegulatorARVINDNo ratings yet
- INGOLD, Tim. Perceiving The EnviromentDocument15 pagesINGOLD, Tim. Perceiving The EnviromentCassiana Oliveira da SilvaNo ratings yet
- Gas Leakage Detection Using Arm7 and ZigbeeDocument18 pagesGas Leakage Detection Using Arm7 and ZigbeevinjamurisivaNo ratings yet
- MD Nastran R3 - Explicit Nonlinear SOL 700 User's Guide PDFDocument602 pagesMD Nastran R3 - Explicit Nonlinear SOL 700 User's Guide PDFpezz07No ratings yet
- OP5142 User Manual-ADocument40 pagesOP5142 User Manual-AJignesh MakwanaNo ratings yet
- Radio - Micro - Bit RuntimeDocument16 pagesRadio - Micro - Bit RuntimeJohn WestNo ratings yet
- Types of Machine DrawingDocument19 pagesTypes of Machine DrawingAmexTesfayeKora100% (5)
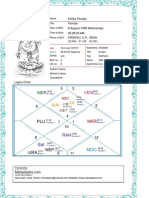
- Kritika Pandey (Kaushambi)Document15 pagesKritika Pandey (Kaushambi)nishink9No ratings yet
- Manual HDCVI DVR SeriesDocument144 pagesManual HDCVI DVR SerieshansturNo ratings yet
- ROBT308Lecture22Spring16 PDFDocument52 pagesROBT308Lecture22Spring16 PDFrightheartedNo ratings yet
- Bonus, Alexander Evan - The Metronomic Performance Practice - A History of Rhythm, Metronomes, and The Mechanization of MusicalityDocument597 pagesBonus, Alexander Evan - The Metronomic Performance Practice - A History of Rhythm, Metronomes, and The Mechanization of MusicalityNoMoPoMo576100% (2)
- Human BehaviorDocument14 pagesHuman BehaviorJay Ann AguilarNo ratings yet
- CV Europass 20190114 LucianConstantin enDocument2 pagesCV Europass 20190114 LucianConstantin enLucian DumitracheNo ratings yet
- Polite Form and Verb Stems: Not Being Rude in JapanDocument84 pagesPolite Form and Verb Stems: Not Being Rude in Japaneulea larkaroNo ratings yet
- Midas Manual PDFDocument49 pagesMidas Manual PDFNishad Kulkarni100% (1)
- Full Download Strategic Management Text and Cases 9th Edition Dess Test BankDocument35 pagesFull Download Strategic Management Text and Cases 9th Edition Dess Test Banksaumvirgen2375812100% (28)
- Course 5 - Cooperative Principle and ImplicatureDocument6 pagesCourse 5 - Cooperative Principle and ImplicatureAnca Ionela ManoleNo ratings yet
- Academic Misconduct PolicyDocument29 pagesAcademic Misconduct PolicySahil BatraNo ratings yet
- BehaviourDocument16 pagesBehaviourIshita JainNo ratings yet
- 3412 Timing CalibrationDocument4 pages3412 Timing CalibrationHrvoje Škarica100% (3)
- STAT1008 Cheat SheetDocument1 pageSTAT1008 Cheat SheetynottripNo ratings yet
- Poly Suga BetaineDocument4 pagesPoly Suga Betainemndmatt100% (1)
- B1 IF-Clauses IF006: WWW - English-Practice - atDocument2 pagesB1 IF-Clauses IF006: WWW - English-Practice - atAyeshaNo ratings yet
- 21 Clever Ways To Make Him Chase YouDocument1 page21 Clever Ways To Make Him Chase YouMagdalena SekulovaNo ratings yet
- The Context Switch in FreeRTOS On A Cortex MDocument13 pagesThe Context Switch in FreeRTOS On A Cortex MKristof MulierNo ratings yet
- Technical Data Speedmaster CX 75Document2 pagesTechnical Data Speedmaster CX 75fongkieNo ratings yet
- Prelims Coe Elec2Document72 pagesPrelims Coe Elec2Sheena SapuayNo ratings yet