You might also like
- DRUG ERUPTION GUIDEDocument46 pagesDRUG ERUPTION GUIDESyahDikaNo ratings yet
- Acute Pulmonary Edema - NEJMDocument4 pagesAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- 194 Surgical Cases PDFDocument160 pages194 Surgical Cases PDFkint100% (4)
- Timebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisFrom EverandTimebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisRating: 3.5 out of 5 stars3.5/5 (2)
- Diabetes Melitus: Dr. Ihsanil Husna, SPPDDocument67 pagesDiabetes Melitus: Dr. Ihsanil Husna, SPPDnathan timothyNo ratings yet
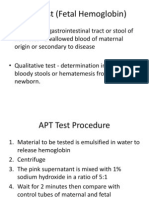
- APT Test (Fetal Hemoglobin)Document11 pagesAPT Test (Fetal Hemoglobin)Diovic TanNo ratings yet
- K4. Diagnosis Holistik - EngDocument21 pagesK4. Diagnosis Holistik - EngBevila KorspoilvilNo ratings yet
- Icd XDocument3 pagesIcd XR Ghianesya GantinaNo ratings yet
- Daftar Kode Diagnosa & TindakanDocument7 pagesDaftar Kode Diagnosa & Tindakannovi andriyaniNo ratings yet
- Kuliah 16 Cor PulmonaleDocument41 pagesKuliah 16 Cor PulmonalecaturwiraNo ratings yet
- Children With Henoch Schonlein Purpura 2.0Document13 pagesChildren With Henoch Schonlein Purpura 2.0soniaNo ratings yet
- Anemia E.C Hematemesis Melena E.C Suspect Gastritis ErrosiveDocument37 pagesAnemia E.C Hematemesis Melena E.C Suspect Gastritis ErrosiveAndayanaIdhamNo ratings yet
- Patch Test ROAT PDFDocument9 pagesPatch Test ROAT PDFrochmandrg dokter gigiNo ratings yet
- Journal Reading THT - OMADocument15 pagesJournal Reading THT - OMAIndira MaycellaNo ratings yet
- Refreshing DHFDocument13 pagesRefreshing DHFNia Nurhayati ZakiahNo ratings yet
- Kegawatan Respirasi May2016-FkumyDocument62 pagesKegawatan Respirasi May2016-FkumyAgustina Tri P. DNo ratings yet
- Systemic Lupus Erythematosus: Pathogenesis and Clinical FeaturesDocument30 pagesSystemic Lupus Erythematosus: Pathogenesis and Clinical FeaturesOrion JohnNo ratings yet
- Diabetic Foot: by Myrna Rita PMRDocument33 pagesDiabetic Foot: by Myrna Rita PMRDianNurlitaAnggrainiNo ratings yet
- Management of Fibromyalgia: Key Messages From Recent Evidence Based GuidelinesDocument10 pagesManagement of Fibromyalgia: Key Messages From Recent Evidence Based GuidelinesArizkamhNo ratings yet
- Hipertiroid HarrisonDocument8 pagesHipertiroid HarrisonravenskaNo ratings yet
- Antibiotic Therapy For Peritonitis: Treatment Overview, Spontaneous Bacterial Peritonitis, Secondary and Tertiary PeritonitisDocument7 pagesAntibiotic Therapy For Peritonitis: Treatment Overview, Spontaneous Bacterial Peritonitis, Secondary and Tertiary PeritonitisTias SubagioNo ratings yet
- Tanda dan Komplikasi Perforasi Usus pada Demam TifoidDocument5 pagesTanda dan Komplikasi Perforasi Usus pada Demam TifoidSisca Dwi Agustina0% (1)
- HDDocument23 pagesHDSardjitoNo ratings yet
- Larynx InfectionsDocument28 pagesLarynx InfectionsMuskan GogiaNo ratings yet
- PansitopeniaDocument33 pagesPansitopeniaBrad WrightNo ratings yet
- Osteonecrosis Caput FemurDocument23 pagesOsteonecrosis Caput FemurdrhendyjuniorNo ratings yet
- POMR Diabetic FootDocument2 pagesPOMR Diabetic FootEnQieey UyunkNo ratings yet
- Buku AJar Infeksi Dan Pediatrik Tropis IDAIDocument31 pagesBuku AJar Infeksi Dan Pediatrik Tropis IDAIAndika SiswantaNo ratings yet
- Nephritic Syndrome: Pyuza, MDDocument41 pagesNephritic Syndrome: Pyuza, MDawadh mbaroukNo ratings yet
- Diabetes Management & Insulin InitiationDocument39 pagesDiabetes Management & Insulin InitiationTaufiqurrochman Nur AminNo ratings yet
- Gnaps EmedicineDocument13 pagesGnaps Emedicineharyanti lupitaNo ratings yet
- OsteoporosisDocument57 pagesOsteoporosisViviViviNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Episkleritis N Skleritis EditDocument12 pagesEpiskleritis N Skleritis EditAnonymous HgX3mN1oNo ratings yet
- Serological Markers of HBV InfectionDocument8 pagesSerological Markers of HBV InfectioncristieristiieNo ratings yet
- Clinical Manifestations and Diagnosis of Acute PancreatitisDocument31 pagesClinical Manifestations and Diagnosis of Acute PancreatitisBrian WilliamNo ratings yet
- Kul Sem 4 Heat Stroke N Fever UHT 2016Document63 pagesKul Sem 4 Heat Stroke N Fever UHT 2016NandaSuryaWijayaNo ratings yet
- Lutembacher's Syndrome at KolonodaleDocument7 pagesLutembacher's Syndrome at KolonodaleWayan GunawanNo ratings yet
- Overview of The Mucopolysaccharidoses: RheumatologyDocument9 pagesOverview of The Mucopolysaccharidoses: RheumatologyLaura Orjuela MateusNo ratings yet
- Kolestasis Intrahepatal Vs EkstrahepatalDocument4 pagesKolestasis Intrahepatal Vs EkstrahepatalrikarikaNo ratings yet
- Disentri Et Causa Bacteria: Jl. Kutai Raya, Perumnas-3, Tangerang Kecamatan Curug, Kab. Tangerang, Provinsi Banten)Document14 pagesDisentri Et Causa Bacteria: Jl. Kutai Raya, Perumnas-3, Tangerang Kecamatan Curug, Kab. Tangerang, Provinsi Banten)Denny LeeNo ratings yet
- Cerebral Malaria Diagnosis & TreatmentDocument42 pagesCerebral Malaria Diagnosis & TreatmentLivia HanisamurtiNo ratings yet
- Drug EruptionDocument46 pagesDrug EruptionSisca ChearzNo ratings yet
- Interpretasi EKG Claudio Per 14 April 2019Document39 pagesInterpretasi EKG Claudio Per 14 April 2019Claudio AgustinoNo ratings yet
- Congenital Adrenal HyperplasiaDocument2 pagesCongenital Adrenal HyperplasiaesyNo ratings yet
- BMI-for-age GIRLS: Birth To 5 Years (Z-Scores)Document15 pagesBMI-for-age GIRLS: Birth To 5 Years (Z-Scores)bonitaNo ratings yet
- Tatalaksana Awal Koreksi Cairan pada Kasus SyokDocument60 pagesTatalaksana Awal Koreksi Cairan pada Kasus Syokmuhammad benyNo ratings yet
- AKI & Indikasi CRRTDocument25 pagesAKI & Indikasi CRRTMaya Sari BaharumNo ratings yet
- Management of Local Anaesthetic Toxicity Update 2009Document6 pagesManagement of Local Anaesthetic Toxicity Update 2009leviosagalNo ratings yet
- TiroidDocument26 pagesTiroidJoni Riana MustaqimNo ratings yet
- Hurler Syndrome (Biochem Repot)Document5 pagesHurler Syndrome (Biochem Repot)Kristine Abegail CantillerNo ratings yet
- Radiologis Gambaran Infeksi Tulang dan FrakturDocument25 pagesRadiologis Gambaran Infeksi Tulang dan FrakturAnonymous HAbhRTs2TfNo ratings yet
- Acute Gastroenteritis (AGE)Document37 pagesAcute Gastroenteritis (AGE)Sari HariyaniNo ratings yet
- Konsensus HipertiroidDocument6 pagesKonsensus HipertiroidDiethaKusumaningrumNo ratings yet
- Critical Appraisal KADocument35 pagesCritical Appraisal KAKentVilandkaNo ratings yet
- Idiopathic Thrombocytopenic Purpura Henoch-Schönlein PurpuraDocument1 pageIdiopathic Thrombocytopenic Purpura Henoch-Schönlein PurpuraMadelyn MedlingNo ratings yet
- Jessica Reid-Adam: Department of Pediatrics, Icahn School of Medicine at Mount Sinai, New York, NYDocument3 pagesJessica Reid-Adam: Department of Pediatrics, Icahn School of Medicine at Mount Sinai, New York, NYAnastasia Widha SylvianiNo ratings yet
- Henoch-Schonlein PurpuraDocument5 pagesHenoch-Schonlein PurpuraPramita Pramana100% (1)
- Brief: Henoch-Schönlein PurpuraDocument5 pagesBrief: Henoch-Schönlein PurpuraAdrian KhomanNo ratings yet
- 2Document5 pages2Manthan PatelNo ratings yet
- Stigma, Discrimination and Living With Hiv/Aids: Pranee Liamputtong EditorDocument425 pagesStigma, Discrimination and Living With Hiv/Aids: Pranee Liamputtong Editorsetyo100% (1)
- Clove Overview of Potential Health Benefits.9Document18 pagesClove Overview of Potential Health Benefits.9Dr-Akash SanthoshNo ratings yet
- Heart Disease in PregnancyDocument20 pagesHeart Disease in PregnancyAnironOrionNo ratings yet
- Circadian Mechanisms in Medicine: Review ArticleDocument12 pagesCircadian Mechanisms in Medicine: Review ArticleNhien TranNo ratings yet
- CME 16 CREDITSDocument6 pagesCME 16 CREDITSAlina LazarNo ratings yet
- Diagnosis of Delirium and Confusional States - UpToDateDocument29 pagesDiagnosis of Delirium and Confusional States - UpToDateLilasNo ratings yet
- Hospital Guidelines - Chaaria MIssion Hospital (Prima Parte)Document10 pagesHospital Guidelines - Chaaria MIssion Hospital (Prima Parte)chaariaNo ratings yet
- Module 3: Clinical PharmacyDocument11 pagesModule 3: Clinical PharmacySelena MoonNo ratings yet
- Drug Formulary For Putatan Health Clinic 2023Document44 pagesDrug Formulary For Putatan Health Clinic 2023colonel555No ratings yet
- 2 Parasitology Parasitic AmoebasDocument8 pages2 Parasitology Parasitic AmoebasknkjnNo ratings yet
- Principles and Concepts of Behavioral Medicine 2018Document1,132 pagesPrinciples and Concepts of Behavioral Medicine 2018Koliber CR100% (1)
- Dextrose in Water (50%)Document2 pagesDextrose in Water (50%)jbambaoNo ratings yet
- Salbutamol StudyDocument2 pagesSalbutamol Studyian100% (1)
- Corona Virus Complete ProjectDocument20 pagesCorona Virus Complete ProjectSantosh Mohapatra100% (1)
- Regional Migratory Osteoporosis of The Knee: A Literature OverviewDocument6 pagesRegional Migratory Osteoporosis of The Knee: A Literature OverviewRobert Partarrieu StegmeierNo ratings yet
- Methodological Instructions - Module 2Document60 pagesMethodological Instructions - Module 2Frt TrfNo ratings yet
- Anaemia of chronic renal diseaseDocument9 pagesAnaemia of chronic renal diseaseVitabuNo ratings yet
- Pao NCPDocument3 pagesPao NCPJay VillasotoNo ratings yet
- Suspected German ISIS Fighter Seized in Mosul May Be Missing 16-Year-Old GirlDocument4 pagesSuspected German ISIS Fighter Seized in Mosul May Be Missing 16-Year-Old GirlSaskia LagemanNo ratings yet
- CholesteatomaDocument2 pagesCholesteatomajljoioiuNo ratings yet
- Cardiovascular DiseaseDocument73 pagesCardiovascular DiseaseAli SherNo ratings yet
- Differential Diagnosis of Bipolar II Disorder and Borderline Personality DisorderDocument11 pagesDifferential Diagnosis of Bipolar II Disorder and Borderline Personality DisorderManu Cortes OsorioNo ratings yet
- Association Between Vitamin D and Systemic Lupus Erythematosus Disease Activity Index in Children and Adolescents - A Systematic Review and Meta-AnalysisDocument9 pagesAssociation Between Vitamin D and Systemic Lupus Erythematosus Disease Activity Index in Children and Adolescents - A Systematic Review and Meta-AnalysiswatiNo ratings yet
- NCP Deficient Fluid VolumeDocument3 pagesNCP Deficient Fluid VolumeDoneva Lyn MedinaNo ratings yet
- The Emotional Impact of Chronic and Disabling Skin Disease - 2005 - DermatologicDocument9 pagesThe Emotional Impact of Chronic and Disabling Skin Disease - 2005 - DermatologicMilena MonteiroNo ratings yet
- Aripiprazole - Mechanism of Action, Clinical Efficacy and Side EffectsDocument10 pagesAripiprazole - Mechanism of Action, Clinical Efficacy and Side EffectsRuben Del CidNo ratings yet
- Mankekar - Implantablehearing Devices Other Than Cochlear ImplantsDocument119 pagesMankekar - Implantablehearing Devices Other Than Cochlear ImplantscetristanNo ratings yet
- AS Level - Infectious Diseases (CH10) Summarised NotesDocument31 pagesAS Level - Infectious Diseases (CH10) Summarised NotesRishika Pasupulati100% (1)
- Diagnostic Therapeutic Algorithms in Internal Medicine For Dogs and CatsDocument529 pagesDiagnostic Therapeutic Algorithms in Internal Medicine For Dogs and Catsluisfilipesilvamoreira19No ratings yet
- NCP Drug StudyDocument8 pagesNCP Drug StudydennisNo ratings yet