You might also like
- Surface Epithelial-Stromal TumorDocument7 pagesSurface Epithelial-Stromal Tumordger11No ratings yet
- Allergic Bronchopulmonary AspergillosisDocument6 pagesAllergic Bronchopulmonary Aspergillosisdger11No ratings yet
- Klyosov 1Document31 pagesKlyosov 1dger11No ratings yet
- Translocations Small00center10 765849Document5 pagesTranslocations Small00center10 765849dger11No ratings yet
- The Flyting of Dunbar and KennedyDocument25 pagesThe Flyting of Dunbar and KennedyCholo MercadoNo ratings yet
- Vertically Transmitted InfectionDocument6 pagesVertically Transmitted Infectiondger11No ratings yet
- Translocations Small00center10 765849Document5 pagesTranslocations Small00center10 765849dger11No ratings yet
- Squamous Cell Carcinoma of The LungDocument2 pagesSquamous Cell Carcinoma of The Lungdger11No ratings yet
- Medullary Thyroid CancerDocument5 pagesMedullary Thyroid Cancerdger11No ratings yet
- Deci Dual IzationDocument2 pagesDeci Dual Izationdger11No ratings yet
- Nodular Fasciitis: Etiology and Clinical CourseDocument3 pagesNodular Fasciitis: Etiology and Clinical Coursedger11No ratings yet
- Luntz Wexner AnalysisDocument17 pagesLuntz Wexner Analysisdger11No ratings yet
- Translocations Small00center10 765849Document5 pagesTranslocations Small00center10 765849dger11No ratings yet
- Congenital Cytomegalovirus InfectionDocument5 pagesCongenital Cytomegalovirus Infectiondger11No ratings yet
- Cancer SyndromeDocument6 pagesCancer Syndromedger11No ratings yet
- Pneumocystis Pneumonia Diagnosis and TreatmentDocument5 pagesPneumocystis Pneumonia Diagnosis and Treatmentdger11No ratings yet
- Atrophic VaginitisDocument3 pagesAtrophic Vaginitisdger11No ratings yet
- Medullary Thyroid CancerDocument5 pagesMedullary Thyroid Cancerdger11No ratings yet
- Squamous Cell Carcinoma of The LungDocument2 pagesSquamous Cell Carcinoma of The Lungdger11No ratings yet
- Congenital Cytomegalovirus InfectionDocument5 pagesCongenital Cytomegalovirus Infectiondger11No ratings yet
- Vertically Transmitted InfectionDocument6 pagesVertically Transmitted Infectiondger11No ratings yet
- Renal Cell CarcinomaDocument15 pagesRenal Cell Carcinomadger11No ratings yet
- Allergic Bronchopulmonary AspergillosisDocument6 pagesAllergic Bronchopulmonary Aspergillosisdger11No ratings yet
- Anglo SaxonDocument4 pagesAnglo Saxondger11No ratings yet
- Viking00barr BWDocument154 pagesViking00barr BWdger11No ratings yet
- Vuk Stefanovic Karadzic: Srpski Rjecnik (1898)Document935 pagesVuk Stefanovic Karadzic: Srpski Rjecnik (1898)krca100% (2)
- Outlines in PathologyDocument200 pagesOutlines in PathologyLisztomaniaNo ratings yet
- The Flyting of Dunbar and KennedyDocument25 pagesThe Flyting of Dunbar and KennedyCholo MercadoNo ratings yet
- Calender of The Close RollsDocument938 pagesCalender of The Close Rollsdger11No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Kegel ExercisesDocument3 pagesKegel ExercisesfynneroNo ratings yet
- UNIT 5 THE EXCRETORY SYSTEM DefDocument3 pagesUNIT 5 THE EXCRETORY SYSTEM DefShalini Hotwani NathaniNo ratings yet
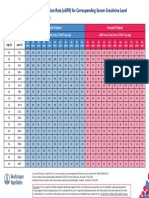
- Egfr ChartDocument1 pageEgfr ChartMahesh DoshiNo ratings yet
- Infectious Causes of Dysuria in Adult MenDocument5 pagesInfectious Causes of Dysuria in Adult MenFrancisco Javier Contreras MoralesNo ratings yet
- Cystitis & UrethritisDocument13 pagesCystitis & UrethritisfemmyNo ratings yet
- Piuria EsterilDocument4 pagesPiuria EsterilBruno Vilela MonteiroNo ratings yet
- (2017) Bladder BrachyDocument7 pages(2017) Bladder BrachyStirNo ratings yet
- Cambridge Urology MCQDocument37 pagesCambridge Urology MCQManju85% (13)
- Lecture 2 - Anatomy of The Ureters, Bladder and UrethraDocument7 pagesLecture 2 - Anatomy of The Ureters, Bladder and UrethraNatalie LiNo ratings yet
- Brosur Cusa Clarity KomplitDocument11 pagesBrosur Cusa Clarity KomplitrossiNo ratings yet
- Final - Susunan Acara Simposium Sehari Urologi Updated Untuk Dokter UmumDocument1 pageFinal - Susunan Acara Simposium Sehari Urologi Updated Untuk Dokter UmumRindy NugraeniNo ratings yet
- Foley Catheterization Insertion and RemovalDocument5 pagesFoley Catheterization Insertion and RemovalArmySapphireNo ratings yet
- Condom For Male and FemaleDocument3 pagesCondom For Male and FemaledeliejoyceNo ratings yet
- Excretion in Human BeingsDocument2 pagesExcretion in Human BeingsDwi Apriyanti SumantriNo ratings yet
- Persuasive Preparation OutlineDocument2 pagesPersuasive Preparation Outlineapi-490667843No ratings yet
- Renal MCQ GuideDocument10 pagesRenal MCQ GuideahmedNo ratings yet
- Yusriani Muslimin, Wahyuni Arif, Resty RyadinencyDocument7 pagesYusriani Muslimin, Wahyuni Arif, Resty RyadinencyZainNo ratings yet
- Male Human Sexual Anatomy SoftDocument6 pagesMale Human Sexual Anatomy SoftKlaire Ira SantosNo ratings yet
- Pae PutiDocument3 pagesPae Putimadimadi11No ratings yet
- Pudhucherry Jipmer DoctorsDocument6 pagesPudhucherry Jipmer DoctorsCHANDRAN MAHANo ratings yet
- STORAGE OF SPERM ERECTION OF PenisDocument12 pagesSTORAGE OF SPERM ERECTION OF PenisAkhand PratapNo ratings yet
- Further - Hospital List - 022021 - Master - EngDocument5 pagesFurther - Hospital List - 022021 - Master - EngCarmen UngureanuNo ratings yet
- Sex Stories IndonesiaDocument3 pagesSex Stories IndonesiausahamerekaNo ratings yet
- Natural Penis Enlargement Exercises 1 PDFDocument12 pagesNatural Penis Enlargement Exercises 1 PDFCatherine Mic100% (5)
- List of Empanelled HospitalsDocument17 pagesList of Empanelled Hospitalsfathima555100% (1)
- Measuring Quality of Urology Care Using A Qualified Clinical Data RegistryDocument11 pagesMeasuring Quality of Urology Care Using A Qualified Clinical Data RegistryphoenixibexNo ratings yet
- Cottenden - Wagg - Supplementary - 23551 ASW Edited Again PDFDocument74 pagesCottenden - Wagg - Supplementary - 23551 ASW Edited Again PDFrohiniNo ratings yet
- Female Condome How To UseDocument4 pagesFemale Condome How To UseRam Bahadur Saru100% (4)
- How to Have Safer Anal SexDocument2 pagesHow to Have Safer Anal SexTech On Demand Solution ProvidersNo ratings yet
- 3Document13 pages3Urologi Unpad Februari 2023No ratings yet