You might also like
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Growth Hormone DisordersDocument1 pageGrowth Hormone DisordersVishalNo ratings yet
- Prioritization LectureDocument6 pagesPrioritization LecturesamNo ratings yet
- Visual Chart 2 - Developmental MilestonesDocument1 pageVisual Chart 2 - Developmental MilestonesVishalNo ratings yet
- NCLEX Cram SheetDocument6 pagesNCLEX Cram Sheetaishwariyapokharel55No ratings yet
- Asthma - Pathom, Signs & ComlicationsDocument1 pageAsthma - Pathom, Signs & ComlicationsVishalNo ratings yet
- 31 Acid Base Imbalances ABGs II - 230110 - 004938Document2 pages31 Acid Base Imbalances ABGs II - 230110 - 004938JanaNo ratings yet
- 11 Diabetic FootDocument37 pages11 Diabetic Footkim suhoNo ratings yet
- Hematologic DisordersDocument32 pagesHematologic DisordersQuolette ConstanteNo ratings yet
- Cardiac PathophysiologyDocument36 pagesCardiac Pathophysiologykim suhoNo ratings yet
- Basic Chart 1 of 2 - Delopmental MilestonesDocument1 pageBasic Chart 1 of 2 - Delopmental MilestonesVishalNo ratings yet
- Concept Map CholesectomyDocument3 pagesConcept Map CholesectomyDoreen Claire100% (1)
- OB Quizlet3 Nursing Care of ChildrenDocument6 pagesOB Quizlet3 Nursing Care of ChildrenDanielle ShullNo ratings yet
- Allergies chart documentation guideDocument2 pagesAllergies chart documentation guideVictoriaStoneHarrisNo ratings yet
- Labor ReadinessDocument1 pageLabor ReadinessEvidence ChaibvaNo ratings yet
- Pediatric Pharmacology 07Document45 pagesPediatric Pharmacology 07Nadz CyNo ratings yet
- Completed Concept MapDocument4 pagesCompleted Concept Mapapi-607361848No ratings yet
- Concept MapDocument5 pagesConcept Mapapi-546509005No ratings yet
- Sbar 2011Document2 pagesSbar 2011Brian Esser100% (1)
- Care of Patients with Musculoskeletal TraumaDocument7 pagesCare of Patients with Musculoskeletal TraumaJosephine Navarro100% (1)
- Musculoskeletal disorders in childrenDocument73 pagesMusculoskeletal disorders in childrenMuhammadNo ratings yet
- Nclex-Rn CramsheetDocument2 pagesNclex-Rn Cramsheetapi-287105616No ratings yet
- NUR 200 Tanner's Model - Noticing Through Reflecting-Updated 2020Document4 pagesNUR 200 Tanner's Model - Noticing Through Reflecting-Updated 2020Oliver NamyaloNo ratings yet
- HypertensionDocument52 pagesHypertensionWahyunitadotokaNo ratings yet
- Maternal Ob NotesDocument103 pagesMaternal Ob NotesBoris OrbetaNo ratings yet
- Fundamentals of Nursing - by Darius CandelarioDocument332 pagesFundamentals of Nursing - by Darius CandelarioEmman RamosNo ratings yet
- Communicating With Distress Patient and Family - DR Loh Ee ChinDocument20 pagesCommunicating With Distress Patient and Family - DR Loh Ee Chinmalaysianhospicecouncil6240100% (1)
- Parenting Styles: - Dictatorial or AuthoritarianDocument45 pagesParenting Styles: - Dictatorial or AuthoritarianCourseTree LearningNo ratings yet
- Prof. Sandra M. Covarrubias - September 24, 2021: 5.2fluid & Electrolytes ImbalancesDocument5 pagesProf. Sandra M. Covarrubias - September 24, 2021: 5.2fluid & Electrolytes ImbalancesIvy VillalobosNo ratings yet
- Flash Cards Vocab For Exam 1. Jarvis CH 1-3, 8, 9, 12, 13http - P.quizlet - Com - Settitle Health Assessment Vocab For Exam 1Document22 pagesFlash Cards Vocab For Exam 1. Jarvis CH 1-3, 8, 9, 12, 13http - P.quizlet - Com - Settitle Health Assessment Vocab For Exam 1tipredd100% (1)
- Presented By: Anjani.S.Kamal 1 Year MSC (N)Document23 pagesPresented By: Anjani.S.Kamal 1 Year MSC (N)shubham vermaNo ratings yet
- Hesi Management of A Medical UnitDocument2 pagesHesi Management of A Medical UnitAna Bienne100% (1)
- Unit 1 Definitions/key Terms Varcarolis Mental Health NursingDocument6 pagesUnit 1 Definitions/key Terms Varcarolis Mental Health Nursingatl_nurse_studentNo ratings yet
- HemiplegiaDocument17 pagesHemiplegiaStefany CelineNo ratings yet
- BSN Reflective Journal on Postpartum Hemorrhage ScenarioDocument2 pagesBSN Reflective Journal on Postpartum Hemorrhage ScenarioJennifer Goodlet100% (1)
- Behavioral Health Care PlanDocument12 pagesBehavioral Health Care Planapi-520841770100% (1)
- Amniotic Band SyndromeDocument47 pagesAmniotic Band SyndromeNazrul Islam JhinukNo ratings yet
- Delfinm QsenDocument57 pagesDelfinm Qsenapi-346220114No ratings yet
- Nclex-Overview: National Council Licensure ExaminationDocument13 pagesNclex-Overview: National Council Licensure ExaminationNaufal Fadli AmzarNo ratings yet
- Ch34 PharmDocument8 pagesCh34 PharmShaneka WilliamsNo ratings yet
- Adult Health III Final Study GuideDocument12 pagesAdult Health III Final Study GuideRyanne JNo ratings yet
- Function of G I System: The Primary Digestive Functions Are Break Down Food Particles "Document113 pagesFunction of G I System: The Primary Digestive Functions Are Break Down Food Particles "cherryann_12100% (1)
- Global Nursing Pediatrics. Nclex - RNDocument14 pagesGlobal Nursing Pediatrics. Nclex - RNNANANo ratings yet
- Kaplan Full Lenth Remember SheetDocument7 pagesKaplan Full Lenth Remember SheetbinaryfizzNo ratings yet
- Cardiac Mnemonics/ Memory CardsDocument35 pagesCardiac Mnemonics/ Memory CardsLids70No ratings yet
- Fundamentals of Nursing PDocument31 pagesFundamentals of Nursing Papi-26587879100% (4)
- HemaDocument15 pagesHemauzbekistan143No ratings yet
- Developmental Stages from Infancy to AdolescenceDocument6 pagesDevelopmental Stages from Infancy to AdolescenceGeguirra, Michiko SarahNo ratings yet
- Antidepressant Cheat Sheet: TCA Ssri SnriDocument1 pageAntidepressant Cheat Sheet: TCA Ssri SnriLillianNo ratings yet
- Acetaminophen PDFDocument1 pageAcetaminophen PDFmp1757No ratings yet
- SBARQ FormDocument1 pageSBARQ FormTracy100% (5)
- Psoriatic ArthritisDocument12 pagesPsoriatic ArthritisSelvia RosadiNo ratings yet
- Review of Systems ANDREADocument7 pagesReview of Systems ANDREAAndrea Dora OrtalizNo ratings yet
- WWW - Qworld.co - in A-Z Disease List For NEETPG: IF Vit B Megaloblastic Anemia)Document5 pagesWWW - Qworld.co - in A-Z Disease List For NEETPG: IF Vit B Megaloblastic Anemia)Qworld100% (1)
- Acid Base Balance: Carol Johns, MSN, RNDocument36 pagesAcid Base Balance: Carol Johns, MSN, RNkatrinasdNo ratings yet
- Pediatric NursingDocument17 pagesPediatric NursingMark Ray A. EspinozaNo ratings yet
- Enuresis in Children - A Case - Based ApproachDocument9 pagesEnuresis in Children - A Case - Based ApproachBogdan NeamtuNo ratings yet
- Pediatrics Kyle NotesDocument20 pagesPediatrics Kyle NotesBrittany Miley100% (1)
- Health AssessmentDocument17 pagesHealth AssessmentNina OaipNo ratings yet
- Assessment and Management of Patients With Endocrine DisordersDocument78 pagesAssessment and Management of Patients With Endocrine Disordershenny1620100% (1)
- Disorders of The EarDocument7 pagesDisorders of The Earhenny1620No ratings yet
- Mce CODocument24 pagesMce COMieh PacualNo ratings yet
- Fluids&ElectrolytesDocument59 pagesFluids&Electrolyteshenny1620No ratings yet
- Lectures First WeekDocument16 pagesLectures First Weekhenny1620No ratings yet
- Gyn 9 - All Gynecology 5 2021Document22 pagesGyn 9 - All Gynecology 5 2021Menna Kamal100% (3)
- FengShui Inspection IDocument52 pagesFengShui Inspection IDavid Hu100% (3)
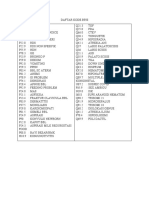
- Daftar Kode BPJSDocument2 pagesDaftar Kode BPJSlilik agustinNo ratings yet
- Could Neurological Illness Have Infuenced Goyas Pictorial StyleDocument9 pagesCould Neurological Illness Have Infuenced Goyas Pictorial StyleHudson AlieeNo ratings yet
- Non Follicular PyodermaDocument1 pageNon Follicular PyodermaMagNo ratings yet
- Understanding Psychosis and SchizophreniaDocument32 pagesUnderstanding Psychosis and SchizophreniaAnonymous zxTFUoqzklNo ratings yet
- Preoperative Testing and Medication ManagementDocument27 pagesPreoperative Testing and Medication ManagementWidya JelitaNo ratings yet
- Neuro-Ophthalmology ICD-10 Quick Reference GuideDocument4 pagesNeuro-Ophthalmology ICD-10 Quick Reference GuideFaisal ApendixNo ratings yet
- 342 MCQDocument4 pages342 MCQRAJESH SHARMA100% (1)
- The Role of Epidemiology in Public HealthDocument19 pagesThe Role of Epidemiology in Public HealthGilbert LimenNo ratings yet
- Therapy PulmonologyDocument22 pagesTherapy PulmonologyCavinpal SinghNo ratings yet
- Risk Factors and Teaching for Laryngeal Cancer PatientDocument2 pagesRisk Factors and Teaching for Laryngeal Cancer Patientatarisgurl08100% (1)
- Granulomatous InflammationDocument20 pagesGranulomatous InflammationPradeep100% (3)
- Effect of Physiotherapy Rehabilitation On Volkmann Ischemic Contracture-A Case StudyDocument2 pagesEffect of Physiotherapy Rehabilitation On Volkmann Ischemic Contracture-A Case StudyIntan HaddadNo ratings yet
- Drug laxative reduces ammonia lactuloseDocument6 pagesDrug laxative reduces ammonia lactuloseRj MagalingNo ratings yet
- Family CoDocument52 pagesFamily ComansiagrawalNo ratings yet
- Donatio Mortis CausaDocument6 pagesDonatio Mortis CausaJohn Phelan100% (2)
- PARASITOLOGY (Quizlet)Document9 pagesPARASITOLOGY (Quizlet)Allyssa AniNo ratings yet
- Fundamentals of Nursing 1Document6 pagesFundamentals of Nursing 1Ruel M. BersabeNo ratings yet
- BASIC NUTRITION GUIDELINESDocument7 pagesBASIC NUTRITION GUIDELINESMicko QuintoNo ratings yet
- MCQ Anemia Antiplatelete MalariaDocument5 pagesMCQ Anemia Antiplatelete Malariasherif mamdoohNo ratings yet
- Community PDFDocument12 pagesCommunity PDFJaja D. JimenezNo ratings yet
- Notes On History Taking in The Cardiovascular SystemDocument9 pagesNotes On History Taking in The Cardiovascular Systemmdjohar72100% (1)
- Health FairDocument11 pagesHealth FairThe Lima NewsNo ratings yet
- 2Document43 pages2myNo ratings yet
- Use and AbuseDocument34 pagesUse and AbuseVa KhoNo ratings yet
- Common Foot and Ankle ProblemsDocument62 pagesCommon Foot and Ankle ProblemsYasmeen Bibi100% (1)
- NIRAJ AHUJA PsychiatryDocument268 pagesNIRAJ AHUJA Psychiatrybrij bhushan kumarNo ratings yet
- Photography IsDocument2 pagesPhotography IsRebecca Dela CruzNo ratings yet
- Tinnitus Today December 1998 Vol 23, No 4Document29 pagesTinnitus Today December 1998 Vol 23, No 4American Tinnitus AssociationNo ratings yet