You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- ProsesDocument19 pagesProsesBagas WahyuNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
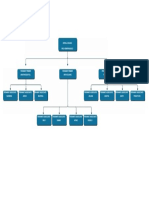
- Struktur OrganisasiDocument1 pageStruktur OrganisasiBagas WahyuNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- JOB APPLICATIONDocument1 pageJOB APPLICATIONBagas WahyuNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Job Application Cover LetterDocument1 pageJob Application Cover LetterBagas WahyuNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Pre Interview DemandDocument3 pagesPre Interview DemandBagas WahyuNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Sample Business Plan TemplateDocument19 pagesSample Business Plan TemplateBagas WahyuNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Surat Dan MemoDocument4 pagesSurat Dan MemoBagas WahyuNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Cancer Lesson Plan For High SchoolDocument7 pagesCancer Lesson Plan For High SchoolUm IbrahimNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- D A Up To 2 YearDocument7 pagesD A Up To 2 YearNischitha G CNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- 4th Quarter CAPSTONEDocument30 pages4th Quarter CAPSTONEWallace RamosNo ratings yet
- CA IC 130LF 14 00 01 en ArxDocument8 pagesCA IC 130LF 14 00 01 en ArxRendy EksaNo ratings yet
- Loxapine Drug StudyDocument5 pagesLoxapine Drug Studyshadow gonzalezNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Summary Water Treatment PlantDocument4 pagesSummary Water Treatment PlantDalil Nur FarahaniNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Bio SaftyDocument7 pagesBio Saftyapi-283956320No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Cipero & Guaracara River Water Quality Site VisitsDocument76 pagesCipero & Guaracara River Water Quality Site VisitsBrandon Atwell79% (29)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- New Consensus On Non Cirrhotic Portal FibrosisDocument41 pagesNew Consensus On Non Cirrhotic Portal Fibrosisramesh5889No ratings yet
- Types of GuidanceDocument13 pagesTypes of GuidanceJomar Gasilla Navarro100% (1)
- 004 General Consent English (Front)Document2 pages004 General Consent English (Front)عبدالله الرعويNo ratings yet
- Monthly Current Affairs Quiz - January 2023: Follow UsDocument244 pagesMonthly Current Affairs Quiz - January 2023: Follow UsSubhankar BasakNo ratings yet
- Msds Coal PDFDocument4 pagesMsds Coal PDFGuntur Wijaya100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Q&A2Document3 pagesQ&A2Marv MarvNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Review Article On Chemical Constituents and Uses of Turmeric PlantDocument8 pagesReview Article On Chemical Constituents and Uses of Turmeric PlantEditor IJTSRDNo ratings yet
- PALLIATIVE CARE SYMPTOM MANAGEMENTDocument153 pagesPALLIATIVE CARE SYMPTOM MANAGEMENTrlinao100% (3)
- Behavioral Health Professionals DirectoryDocument102 pagesBehavioral Health Professionals DirectoryepraetorianNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- TB Teaching PlanDocument5 pagesTB Teaching PlanTrisha Fae Loyola Balagot100% (1)
- Douglas Crucey, A043 446 797 (BIA June 12, 2017)Document20 pagesDouglas Crucey, A043 446 797 (BIA June 12, 2017)Immigrant & Refugee Appellate Center, LLCNo ratings yet
- Hospital Administrative Assistant Resume-A4Document2 pagesHospital Administrative Assistant Resume-A4Philip V AlexNo ratings yet
- OSHS LegislationsDocument59 pagesOSHS LegislationsAlvin DeliroNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Week 1 Day 1Document2 pagesWeek 1 Day 1arens100% (1)
- LVMH - Code of ConductDocument13 pagesLVMH - Code of ConductElena DianaNo ratings yet
- What is pancytopenia and its causesDocument33 pagesWhat is pancytopenia and its causesDabogski FranceNo ratings yet
- Paedo Don TicsDocument103 pagesPaedo Don TicsIana RusuNo ratings yet
- Labor and Delivery QuizDocument7 pagesLabor and Delivery QuizAmy50% (2)
- KAP regarding BSE among womenDocument30 pagesKAP regarding BSE among womenrandika wijesooriyaNo ratings yet
- 31.ergonomic Approach of Modification of Seat - EncDocument11 pages31.ergonomic Approach of Modification of Seat - EncSHASHANK ROHITNo ratings yet
- Middle Childhood Physical Development (6-11 YearsDocument13 pagesMiddle Childhood Physical Development (6-11 YearsAngela YlaganNo ratings yet
- Bailey SafeMedPharmacyTechnicianDocument10 pagesBailey SafeMedPharmacyTechnicianRazak AbdullahNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)