You might also like
- Neurology Multiple Choice Questions With Explanations: Volume IFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IRating: 4 out of 5 stars4/5 (7)
- Dermatological PharmacologyDocument25 pagesDermatological Pharmacologyborneo225100% (1)
- Critical Care Board and Certif StatPearls Publishing LLC 2Document2,019 pagesCritical Care Board and Certif StatPearls Publishing LLC 2Konstantinos IliakopoulosNo ratings yet
- PART 19: Disorders Associated With Environmental Exposures: Altitude IllnessDocument24 pagesPART 19: Disorders Associated With Environmental Exposures: Altitude IllnessjonasNo ratings yet
- Part 15 - Disorders Associated With Environmental ExposuresDocument86 pagesPart 15 - Disorders Associated With Environmental Exposuresnklinh.y2021No ratings yet
- Art 10375 WebDocument8 pagesArt 10375 Websogand2916No ratings yet
- Fisiologia Basica de La AlturaDocument12 pagesFisiologia Basica de La AlturaMARIA MARCELINA PACHECHO VARGASNo ratings yet
- Acute Medical Problems in The Himalayas Outside The Setting of Altitude SicknessDocument8 pagesAcute Medical Problems in The Himalayas Outside The Setting of Altitude SicknessMacho Peruano Que se RespetaNo ratings yet
- Avances en La Prevencion y Tto Mal de Laa AlturasDocument20 pagesAvances en La Prevencion y Tto Mal de Laa AlturasLina María CañónNo ratings yet
- Acute High-Altitude SicknessDocument14 pagesAcute High-Altitude SicknessJoseph AmeerNo ratings yet
- High Altitude IllnessDocument9 pagesHigh Altitude Illnesswana_iswaraNo ratings yet
- Altitude Headache: Uncommon Headache Syndrome (J Ailani, Section Editor)Document5 pagesAltitude Headache: Uncommon Headache Syndrome (J Ailani, Section Editor)Siddharth KharkarNo ratings yet
- Ivanova Z.O. M.D.: High-Altitude Illness. Dysbarism and Decompression SicknessDocument23 pagesIvanova Z.O. M.D.: High-Altitude Illness. Dysbarism and Decompression SicknessVaishali SinghNo ratings yet
- Acute Mountain Sickness: David R. Murdoch and Andrew) - PollardDocument4 pagesAcute Mountain Sickness: David R. Murdoch and Andrew) - PollardCésar LabastidaNo ratings yet
- Za Fren 2014Document11 pagesZa Fren 2014Haydee MogrovejoNo ratings yet
- High Altitude, Heat and Cold Injuries-2Document107 pagesHigh Altitude, Heat and Cold Injuries-2Bismillah LancarNo ratings yet
- High Altitude IllnessesDocument3 pagesHigh Altitude IllnessesMabookgm MaNo ratings yet
- Jurnal AMS PDFDocument8 pagesJurnal AMS PDFputriseptinaNo ratings yet
- The Physiologic Basis of High-Altitude DiseasesDocument12 pagesThe Physiologic Basis of High-Altitude DiseasesMario LosadaNo ratings yet
- Fakultas Kedokteran Universitas Islam Al Azhar: Dr. Dasti Anditiarina, SP - KPDocument30 pagesFakultas Kedokteran Universitas Islam Al Azhar: Dr. Dasti Anditiarina, SP - KPBaiqLinaAnggrianNo ratings yet
- Anaphylaxis: Diagnosis and Management: Mja Practice Essentials - AllergyDocument7 pagesAnaphylaxis: Diagnosis and Management: Mja Practice Essentials - AllergyFran ramos ortegaNo ratings yet
- Dapus 32Document4 pagesDapus 32Titi SulistiowatiNo ratings yet
- High Altitude IllnessDocument18 pagesHigh Altitude IllnessElmer VasquezNo ratings yet
- Acetazolamide: A Treatment For Chronic Mountain SicknessDocument7 pagesAcetazolamide: A Treatment For Chronic Mountain Sicknessyuddy Fabiola Equiza BarrosoNo ratings yet
- Anaphylaxis Diagnosis and ManagementDocument10 pagesAnaphylaxis Diagnosis and Managementd dNo ratings yet
- Altitude Illness - Risk Factors, Prevention, Presentation, and TreatmentDocument8 pagesAltitude Illness - Risk Factors, Prevention, Presentation, and TreatmentVenansius Ratno KurniawanNo ratings yet
- Dysnatremia in The ICU: Milap Pokaharel and Clay A. BlockDocument13 pagesDysnatremia in The ICU: Milap Pokaharel and Clay A. BlockJonathan Gustavo MenaNo ratings yet
- Demystifying HyponatremiaDocument10 pagesDemystifying HyponatremiaJavier Vivanco100% (1)
- Acute ComaDocument16 pagesAcute ComaDean AccountNo ratings yet
- Pathophysiology and Etiology of Edema in AdultsDocument15 pagesPathophysiology and Etiology of Edema in AdultsJovie Anne CabangalNo ratings yet
- Coma MixedematososDocument8 pagesComa Mixedematososisabella jimenez cadavidNo ratings yet
- CDC 58372 DS1Document20 pagesCDC 58372 DS1LAURA VANESSA URRUTIA ALVAREZNo ratings yet
- The Management of Vasovagal Syncope: R.A. Kenny and T. McnicholasDocument8 pagesThe Management of Vasovagal Syncope: R.A. Kenny and T. McnicholasKat ZNo ratings yet
- Case PresentationDocument23 pagesCase PresentationSiva Narendra Naidu RangumudriNo ratings yet
- Neuro-Hiponatremia 4Document11 pagesNeuro-Hiponatremia 4Kim Escobedo HurtadoNo ratings yet
- Human Behaviour and Development Under High-Altitude ConditionsDocument11 pagesHuman Behaviour and Development Under High-Altitude ConditionsIsa Hernandez RiveroNo ratings yet
- Circulatory ShockDocument9 pagesCirculatory ShockVictor Euclides Briones MoralesNo ratings yet
- Rhabdomyolysis: Pathogenesis, Diagnosis, and TreatmentDocument12 pagesRhabdomyolysis: Pathogenesis, Diagnosis, and TreatmentSyifaNo ratings yet
- Initial Diagnosis and Management of ComaDocument17 pagesInitial Diagnosis and Management of Comaguugle gogleNo ratings yet
- Altitude - Related Illnesses in Traveler: I K Agus SomiaDocument41 pagesAltitude - Related Illnesses in Traveler: I K Agus SomiaNym Angga SantosaNo ratings yet
- Concise Clinical Review: High-Altitude MedicineDocument9 pagesConcise Clinical Review: High-Altitude MedicineJim Huanuqueño TacuriNo ratings yet
- New MAS HIEDocument37 pagesNew MAS HIEDevuchandana RNo ratings yet
- Role of Chemoreception in Cardiorespiratory Acclimatization To, Anddeacclimatization From, HypoxiDocument9 pagesRole of Chemoreception in Cardiorespiratory Acclimatization To, Anddeacclimatization From, HypoxiAbeer SallamNo ratings yet
- Pi Is 0091674999701065Document9 pagesPi Is 0091674999701065Choirun NisaNo ratings yet
- Altitude Related IllnessDocument8 pagesAltitude Related IllnesscharmdoszNo ratings yet
- Sirs ModsDocument10 pagesSirs ModsRENEROSE TORRESNo ratings yet
- CirculatoryShock NejmraDocument9 pagesCirculatoryShock NejmraMaria Agostina EspecheNo ratings yet
- Anaphylaxis: Diagnosis and Management: The Medical Journal of Australia October 2006Document8 pagesAnaphylaxis: Diagnosis and Management: The Medical Journal of Australia October 2006DidiNo ratings yet
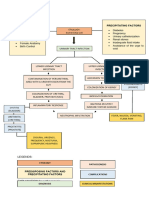
- Massive Intracranial Fluid CollectionDocument29 pagesMassive Intracranial Fluid CollectionAiza QenNo ratings yet
- Key Terms and DefinitionsDocument257 pagesKey Terms and DefinitionslaurafultanoNo ratings yet
- Ventilasi Sungkup SulitDocument22 pagesVentilasi Sungkup SulitNurul FitriNo ratings yet
- Acute High Altitude IllenesDocument9 pagesAcute High Altitude IllenesDiego CastroNo ratings yet
- High Altitude SicknessDocument27 pagesHigh Altitude SicknessMuhammad AleemNo ratings yet
- Respiratory AcidosisDocument5 pagesRespiratory Acidosisapi-376421583% (6)
- Sleep Related Disorder PDFDocument6 pagesSleep Related Disorder PDFmaybel tiwangNo ratings yet
- Neurocardio NursingDocument101 pagesNeurocardio NursingMatt Lao DionelaNo ratings yet
- Inhaled Anesthetics Part 1Document30 pagesInhaled Anesthetics Part 1ashley-keaneNo ratings yet
- Homeopathic High Camp: The Effect of Coca Altitude SicknessDocument11 pagesHomeopathic High Camp: The Effect of Coca Altitude SicknessValerian MendoncaNo ratings yet
- Clinical Disorders Excess Vasopressin/syndrome of Inappropriate Antidiuretic HormoneDocument5 pagesClinical Disorders Excess Vasopressin/syndrome of Inappropriate Antidiuretic HormoneDirgantari PademmeNo ratings yet
- The Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaFrom EverandThe Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaNo ratings yet
- Dem Tickler NotesDocument1 pageDem Tickler NotesSeff CausapinNo ratings yet
- Disorders of The Female Reproductive System PDFDocument4 pagesDisorders of The Female Reproductive System PDFSeff CausapinNo ratings yet
- Thyroid 2Document58 pagesThyroid 2Seff CausapinNo ratings yet
- Approach To Patient With Endocrine DisordersDocument2 pagesApproach To Patient With Endocrine DisordersSeff CausapinNo ratings yet
- Anterior Pituitary Tumor SyndromesDocument10 pagesAnterior Pituitary Tumor SyndromesSeff CausapinNo ratings yet
- Glomerular Diseases: Pathogenesis of Glomerular Diseases Progression of Glomerular DiseasesDocument6 pagesGlomerular Diseases: Pathogenesis of Glomerular Diseases Progression of Glomerular DiseasesSeff CausapinNo ratings yet
- Urinary Tract ObstructionDocument2 pagesUrinary Tract ObstructionSeff CausapinNo ratings yet
- Pathophysiology of SLEDocument16 pagesPathophysiology of SLESeff CausapinNo ratings yet
- Medicine (Dr. Pedroza) Copd 14 FEBRUARY 2018Document3 pagesMedicine (Dr. Pedroza) Copd 14 FEBRUARY 2018Seff CausapinNo ratings yet
- Disturbances in Respiratory FunctionDocument6 pagesDisturbances in Respiratory FunctionSeff CausapinNo ratings yet
- Physical Diagnosis of The ThoraxDocument3 pagesPhysical Diagnosis of The ThoraxSeff Causapin100% (1)
- Complete Guide To Physical ExamDocument19 pagesComplete Guide To Physical ExamSeff Causapin100% (2)
- LeptospirosisDocument2 pagesLeptospirosisSeff CausapinNo ratings yet
- Sympathomimetic Agents: CLIN. PHARM (Dr. Salvador) Asthma 05 SEPT 2017Document3 pagesSympathomimetic Agents: CLIN. PHARM (Dr. Salvador) Asthma 05 SEPT 2017Seff Causapin100% (1)
- Vasoactive PeptidesDocument8 pagesVasoactive PeptidesSeff CausapinNo ratings yet
- Eicosanoids: Arachidonic Acid & Other Polyunsaturated PrecursorsDocument6 pagesEicosanoids: Arachidonic Acid & Other Polyunsaturated PrecursorsSeff CausapinNo ratings yet
- Test Bank On GI PathologyDocument14 pagesTest Bank On GI PathologySeff CausapinNo ratings yet
- Vasoactive PeptidesDocument8 pagesVasoactive PeptidesSeff CausapinNo ratings yet
- HEAD AND NECK 1.robbins & Cotran Pathologic Basis of Disease ReviewerDocument14 pagesHEAD AND NECK 1.robbins & Cotran Pathologic Basis of Disease ReviewerSeff Causapin100% (1)
- SONA ReactionDocument4 pagesSONA ReactionSeff CausapinNo ratings yet
- Summary of Product Characteristics: Concor 5 MG, Film-Coated Tablets Concor 10 MG, Film-Coated TabletsDocument12 pagesSummary of Product Characteristics: Concor 5 MG, Film-Coated Tablets Concor 10 MG, Film-Coated TabletsasdwasdNo ratings yet
- The Human Respiratory System: January 2013Document27 pagesThe Human Respiratory System: January 2013mrkhalid.sobhy67No ratings yet
- Nasaba Magnona Rawan - Cause-Effect Essay Draft 1Document6 pagesNasaba Magnona Rawan - Cause-Effect Essay Draft 1Sami JafarNo ratings yet
- Chapter 28Document13 pagesChapter 28George LeahuNo ratings yet
- Optometry: Accommodative and Binocular Dysfunctions: Prevalence in A Randomised Sample of University StudentsDocument9 pagesOptometry: Accommodative and Binocular Dysfunctions: Prevalence in A Randomised Sample of University StudentsShyannaNo ratings yet
- Orofacial Infections in Children PedoDocument40 pagesOrofacial Infections in Children PedoFourthMolar.comNo ratings yet
- HW 410 Unit 9 Assignment Rhonda Williams 1Document35 pagesHW 410 Unit 9 Assignment Rhonda Williams 1api-441311906No ratings yet
- Pages From Rajesh Bardale Principles of Forensic Medicine and ToxicologyDocument5 pagesPages From Rajesh Bardale Principles of Forensic Medicine and Toxicologymueen hashmiNo ratings yet
- Young - 2007Document21 pagesYoung - 2007TurboNo ratings yet
- Blood and Tissue Flagellates para LecDocument8 pagesBlood and Tissue Flagellates para LecLian MallareNo ratings yet
- 10 11648 J Ajim 20180606 14Document7 pages10 11648 J Ajim 20180606 14Stephanie HellenNo ratings yet
- TungDocument203 pagesTungValdemar Caumo Junior100% (5)
- Xanthogranulomatous Oophoritis Secondary To Talcum Powder Case Report and Review of The LiteratureDocument4 pagesXanthogranulomatous Oophoritis Secondary To Talcum Powder Case Report and Review of The LiteratureCamil ChouairyNo ratings yet
- Nur 111 Session 4 Sas 1Document6 pagesNur 111 Session 4 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Urinary Tract InfectionDocument13 pagesUrinary Tract InfectionMuhamad RockystankiNo ratings yet
- Cerebrum: By: Pedro E. Ampil, M.D.FPSA Department of Human Structural Biology Our Lady of Fatima UniversityDocument29 pagesCerebrum: By: Pedro E. Ampil, M.D.FPSA Department of Human Structural Biology Our Lady of Fatima UniversityPlaza Jeanine LouiseNo ratings yet
- Liver Cirrhosis: DR Alex MogereDocument51 pagesLiver Cirrhosis: DR Alex MogereGladys Maina100% (1)
- 2 PDFDocument297 pages2 PDFTaj KoyyodeNo ratings yet
- Nursing Sensory Perception System Gustatory: Lecturer: Ns. Leni Merdawati, M.KepDocument18 pagesNursing Sensory Perception System Gustatory: Lecturer: Ns. Leni Merdawati, M.KepfaradillaNo ratings yet
- Pathophysiology - UtiDocument2 pagesPathophysiology - UtiAyessa Marie BarbosaNo ratings yet
- Simple Guide Orthopadics Chapter 11 Neurological and Spinal ConditionsDocument86 pagesSimple Guide Orthopadics Chapter 11 Neurological and Spinal ConditionsSurgicalgownNo ratings yet
- Henoch Schonlein Purpura: Dr. Hendratno Halim, Sp. ADocument29 pagesHenoch Schonlein Purpura: Dr. Hendratno Halim, Sp. AYulius Eka Agung Seputra, MSiNo ratings yet
- Bacterial Skin and Soft Tissue Infections: Clinical Review ArticleDocument9 pagesBacterial Skin and Soft Tissue Infections: Clinical Review ArticleRini MayaSariNo ratings yet
- How I Treat Disseminated Intravascular CoagulationDocument10 pagesHow I Treat Disseminated Intravascular CoagulationSergio Alberto Sulub NavarreteNo ratings yet
- Case Based DiscussionDocument62 pagesCase Based DiscussionNeni SetyowatiNo ratings yet
- Cholangiocarcinoma 2 Juni 2018Document40 pagesCholangiocarcinoma 2 Juni 2018Anonymous 1UgsHkUNo ratings yet
- Elsiver NCLEX Critical CareDocument112 pagesElsiver NCLEX Critical CareHasan A AsFour100% (1)
- Kostyev UrologyDocument307 pagesKostyev UrologyBagusNo ratings yet