You might also like
- The GcMAF BookDocument79 pagesThe GcMAF BookVíctor Valdez100% (1)
- Group Imago and The Stages of Group DevelopmentDocument16 pagesGroup Imago and The Stages of Group DevelopmentNarcis Nagy100% (3)
- One Second and A Million Miles - The Bridges of Madison - County - JRBDocument4 pagesOne Second and A Million Miles - The Bridges of Madison - County - JRBKFarnum Jr.0% (6)
- Orthodox America 1794-1976 - Constance J. Tarasar, John H. Erickson, Alexander Doumouras, - 1975 - Orthodox Church America - Anna's ArchiveDocument364 pagesOrthodox America 1794-1976 - Constance J. Tarasar, John H. Erickson, Alexander Doumouras, - 1975 - Orthodox Church America - Anna's ArchivemarcelNo ratings yet
- Anaerobic Digester Design and CalculationDocument41 pagesAnaerobic Digester Design and CalculationJohn TauloNo ratings yet
- Master Kinesiotaping HandoutDocument11 pagesMaster Kinesiotaping HandoutcosasdeangelNo ratings yet
- PEMF ClinicalStudies 1Document38 pagesPEMF ClinicalStudies 1OaNa Miron100% (3)
- Mindful Medical Practice - Clinical Narratives and Therapeutic InsightsDocument169 pagesMindful Medical Practice - Clinical Narratives and Therapeutic InsightsSkg KonNo ratings yet
- Date Performed: August 18, 2015 Group No. and Section: Group 5 WCDE-A Date Submitted: September 1, 2015 Group MembersDocument28 pagesDate Performed: August 18, 2015 Group No. and Section: Group 5 WCDE-A Date Submitted: September 1, 2015 Group MembersCm MacaliaNo ratings yet
- Antibiotic Chart-Infectious Disease Bug Drug Table-2019Document2 pagesAntibiotic Chart-Infectious Disease Bug Drug Table-2019Duy LuuNo ratings yet
- Nhs Bronchiolitis Pathway Acute Setting South East Coast SCNDocument2 pagesNhs Bronchiolitis Pathway Acute Setting South East Coast SCNdrgrizahNo ratings yet
- Cardiovascular Disease Worldwide: Top Causes of Death From CVDDocument1 pageCardiovascular Disease Worldwide: Top Causes of Death From CVDcoloradoresourcesNo ratings yet
- Honest Food GuideDocument1 pageHonest Food Guidepeanutmilk100% (3)
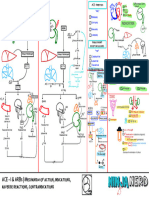
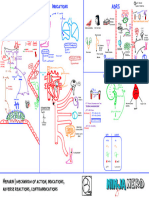
- Cardiovascular Pharmacology) 08 ACE-I - ARBs - KeyDocument1 pageCardiovascular Pharmacology) 08 ACE-I - ARBs - Keyhasanatiya41No ratings yet
- Oral Sur 2 MidtermDocument22 pagesOral Sur 2 Midtermnapat kidsanakaraketNo ratings yet
- IONIX ModelDocument6 pagesIONIX ModelTrường Bửu TrầnNo ratings yet
- ExerciÌ Cio e DCV - Parte 1Document10 pagesExerciÌ Cio e DCV - Parte 1Joao GuimaraesNo ratings yet
- Fever PrimaryCommunityCare Dec 16 FINAL VSDocument2 pagesFever PrimaryCommunityCare Dec 16 FINAL VSnimraNo ratings yet
- Acting Studio Applicaton FormDocument1 pageActing Studio Applicaton ForminfosysofficialhydNo ratings yet
- Health History QuestionnaireDocument4 pagesHealth History QuestionnaireDea Sudiyantika PutriNo ratings yet
- ReferralDocument1 pageReferralmanasabhavaniNo ratings yet
- HypertensionDocument1 pageHypertensionvictor.garcia4080No ratings yet
- Honest Food GuideDocument1 pageHonest Food Guideapi-3714923No ratings yet
- Unending GraceDocument15 pagesUnending GraceMelinda T. Magbanua100% (1)
- HIRADEC Rev April'23 - (REV08)Document10 pagesHIRADEC Rev April'23 - (REV08)DEEPAK MALLIKNo ratings yet
- Telaviv MapDocument1 pageTelaviv Mapshay4323No ratings yet
- Ej 4 Infor PDFDocument1 pageEj 4 Infor PDFJavier RufeteNo ratings yet
- Anthem BassDocument2 pagesAnthem BassRomoliNo ratings yet
- (PIDST) - 391 - Pidst - 20111020114358 - Filejou 2Document20 pages(PIDST) - 391 - Pidst - 20111020114358 - Filejou 2Nareunart KongkaNo ratings yet
- 8 Hullet BrochureDocument19 pages8 Hullet BrochureRonnie TanNo ratings yet
- 8 Hullet BrochureDocument19 pages8 Hullet BrochureRonnie TanNo ratings yet
- Notes AtherosclerosisDocument1 pageNotes AtherosclerosisElizabeth de GuzmanNo ratings yet
- Ujian Patoflow Yola MTDocument1 pageUjian Patoflow Yola MTAdam SipahutarNo ratings yet
- pPYqnlFGTC2UMT6pBejw - 3004-101 Proposed PlansDocument1 pagepPYqnlFGTC2UMT6pBejw - 3004-101 Proposed PlanserniE抖音 AI Mobile Phone Based MovieNo ratings yet
- ANGELES - CANTANDO - ESTAN Final ScoreDocument6 pagesANGELES - CANTANDO - ESTAN Final ScoreSergio FernandezNo ratings yet
- Non Taccostare Allurna Giuseppe Verdi - A MinorDocument5 pagesNon Taccostare Allurna Giuseppe Verdi - A MinorMohammadNo ratings yet
- Health Assessment FormDocument12 pagesHealth Assessment Formmiha3la33No ratings yet
- Vienna Map City CenterDocument1 pageVienna Map City Centeragnes nathaniaNo ratings yet
- Son Tentacion - HeridaDocument12 pagesSon Tentacion - HeridaMauricio AguilarNo ratings yet
- 1 KyrieDocument10 pages1 KyrieRémi TroisgrosNo ratings yet
- Missa Pro Pace: SanctusDocument1 pageMissa Pro Pace: SanctusDawid JuraszekNo ratings yet
- 24x24 AvenzaBasemap TolowaDunesDocument1 page24x24 AvenzaBasemap TolowaDunesMonie DNo ratings yet
- A-01 MergedDocument17 pagesA-01 MergedDeereck Huertas HizoNo ratings yet
- Picu Ready RecknerDocument2 pagesPicu Ready RecknerPranitha Reddy0% (1)
- CH2Document6 pagesCH2fd2m2n8p55No ratings yet
- Nipt TRF MedgenomeDocument4 pagesNipt TRF MedgenomepathbiomedxNo ratings yet
- Given To HospitalityDocument456 pagesGiven To HospitalityBianca PradoNo ratings yet
- Global Report On Birth Defects The Hidden Toll ofDocument1 pageGlobal Report On Birth Defects The Hidden Toll ofvolNo ratings yet
- Rateeatatagh IveDocument424 pagesRateeatatagh IveGeorge TeodorNo ratings yet
- Besame Mucho. Score.Document6 pagesBesame Mucho. Score.AndreiFloreaNo ratings yet
- Head / Hair Face Eyes Nose Oral / Throat Ears Neck: Physical Exam (Heent)Document1 pageHead / Hair Face Eyes Nose Oral / Throat Ears Neck: Physical Exam (Heent)Johnny BeeNo ratings yet
- Mother Gooses Nur 00 ElliDocument128 pagesMother Gooses Nur 00 ElliBranko NikolicNo ratings yet
- Jane Jane: Monday-Sunday/HolidayDocument2 pagesJane Jane: Monday-Sunday/HolidayChristian DominguezNo ratings yet
- Jesus, Etc.: ModeratelyDocument5 pagesJesus, Etc.: ModeratelyBen McMunn100% (1)
- The Structure of Questions in EnglishDocument1 pageThe Structure of Questions in EnglishMohamed NaserNo ratings yet
- Ek Apolas A TB S 2021-22-1Document2 pagesEk Apolas A TB S 2021-22-1Krisztián TóthNo ratings yet
- THC Special OffersDocument2 pagesTHC Special OffersTotalHealthConceptsNo ratings yet
- Cardiovascular Pharmacology) 03 Heparin - KeyDocument1 pageCardiovascular Pharmacology) 03 Heparin - Keyhasanatiya41No ratings yet
- O Praise The Name AnastasisDocument6 pagesO Praise The Name AnastasisFabiana Campanha Veronezi100% (3)
- 13PLAN planMAUGDocument1 page13PLAN planMAUGEvanrey EnriquezNo ratings yet
- Chiquito Team Band - Lejos de TiDocument8 pagesChiquito Team Band - Lejos de TiMercedes Terrón EspinosaNo ratings yet
- It's So Easy Going Green: An Interactive, Scientific Look at Protecting Our EnvironmentFrom EverandIt's So Easy Going Green: An Interactive, Scientific Look at Protecting Our EnvironmentNo ratings yet
- Instant Assessments for Data Tracking, Grade 4: MathFrom EverandInstant Assessments for Data Tracking, Grade 4: MathRating: 5 out of 5 stars5/5 (2)
- Updated Recommendations On The Use of Pneumococcal Vaccines For High-Risk IndividualsDocument5 pagesUpdated Recommendations On The Use of Pneumococcal Vaccines For High-Risk IndividualsyuliNo ratings yet
- Materi I DR HadryastutiDocument38 pagesMateri I DR HadryastutiyuliNo ratings yet
- Appendix7 ChestDrainObsChart F PDFDocument3 pagesAppendix7 ChestDrainObsChart F PDFyuliNo ratings yet
- Hemodinamik SyokDocument15 pagesHemodinamik SyokyuliNo ratings yet
- Ventilation Guidelines For PICU Oct 2010Document13 pagesVentilation Guidelines For PICU Oct 2010MariaUlfaNo ratings yet
- Bookshelf NBK248066 PDFDocument167 pagesBookshelf NBK248066 PDFyuliNo ratings yet
- Febrile NuetropeniaDocument4 pagesFebrile NuetropeniayuliNo ratings yet
- How To Read A Growth Chart - Percentiles ExplainedDocument3 pagesHow To Read A Growth Chart - Percentiles ExplainedyuliNo ratings yet
- 1 Guidelines On Paediatric Parenteral Nutrition.1Document4 pages1 Guidelines On Paediatric Parenteral Nutrition.1titissetiarNo ratings yet
- Cyclophosphamide Treatment in The Oxford Kidney Unit: Renal Unit, Churchill HospitalDocument8 pagesCyclophosphamide Treatment in The Oxford Kidney Unit: Renal Unit, Churchill HospitalyuliNo ratings yet
- A174-05PaedPNGuidel Carbohydrates PDFDocument5 pagesA174-05PaedPNGuidel Carbohydrates PDFyuliNo ratings yet
- PAPER (ENG) - The Early Feeding Skills Assessment For Preterm InfantsDocument15 pagesPAPER (ENG) - The Early Feeding Skills Assessment For Preterm InfantsAldo Hip NaranjoNo ratings yet
- TPN PDFDocument9 pagesTPN PDFyuliNo ratings yet
- Cyclophosphamide Treatment in The Oxford Kidney Unit: Renal Unit, Churchill HospitalDocument8 pagesCyclophosphamide Treatment in The Oxford Kidney Unit: Renal Unit, Churchill HospitalyuliNo ratings yet
- Dialysis Disequilibrium SyndromeDocument8 pagesDialysis Disequilibrium SyndromeyuliNo ratings yet
- Pediatric Nutrition Assessment Final FarahDocument54 pagesPediatric Nutrition Assessment Final Farahyuli0% (1)
- Berrington Gut Microbiota in Preterm Infants Assessment and Relevance To Health and Disease 2012Document7 pagesBerrington Gut Microbiota in Preterm Infants Assessment and Relevance To Health and Disease 2012yuliNo ratings yet
- Incessant VT VFDocument9 pagesIncessant VT VFTor JaNo ratings yet
- Venipuncture (Procedure) : Patrick Kyle C. Ignacio, RRTDocument26 pagesVenipuncture (Procedure) : Patrick Kyle C. Ignacio, RRTCielo DeguzmanNo ratings yet
- TCCC Guidelines August 2011Document12 pagesTCCC Guidelines August 2011OnTheXNo ratings yet
- Philosophy Palliative Care and End of Life Care Per 15-02-2021Document33 pagesPhilosophy Palliative Care and End of Life Care Per 15-02-2021rizki ikhsanNo ratings yet
- Planning Physical Facilities of Hospital and Educational InstitutionDocument5 pagesPlanning Physical Facilities of Hospital and Educational InstitutionSundaraBharathi100% (2)
- Group 1 BARC CaseDocument14 pagesGroup 1 BARC CaseAmbrish ChaudharyNo ratings yet
- Alcohol History Taking - Geeky MedicsDocument6 pagesAlcohol History Taking - Geeky MedicsJahangir AlamNo ratings yet
- Swyer James MacLeod SyndromeDocument12 pagesSwyer James MacLeod Syndromeflori.bNo ratings yet
- Guidebook For Preacc Entrylevelstandards SHCO PDFDocument162 pagesGuidebook For Preacc Entrylevelstandards SHCO PDFArun Kumar100% (3)
- Ambulance Nurse Checklist MMSR2017Document4 pagesAmbulance Nurse Checklist MMSR2017Ahmed OsmanNo ratings yet
- Pelvis Frozen EnglishDocument3 pagesPelvis Frozen EnglishPetar PribicNo ratings yet
- Concept of Disease 1.1 Anatomy and PhysiologyDocument15 pagesConcept of Disease 1.1 Anatomy and PhysiologyAulia SandraNo ratings yet
- Sevrage CannabisDocument29 pagesSevrage CannabismihaelaNo ratings yet
- Appi Psychotherapy 20220018Document8 pagesAppi Psychotherapy 20220018consulta.nicolaslabbeNo ratings yet
- Anesthesia in Dentistry and Extraction of Tooth by Pratyasha ParipurnaDocument42 pagesAnesthesia in Dentistry and Extraction of Tooth by Pratyasha ParipurnapariNo ratings yet
- Samantha Bradley: Work ExperienceDocument3 pagesSamantha Bradley: Work Experienceapi-399988983No ratings yet
- ADN Care Plan - DepressionDocument3 pagesADN Care Plan - DepressionDavid PerezNo ratings yet
- Letter To Stephen Muldrow USAFLM Re Dr. Asad Qamar May-12-2017Document93 pagesLetter To Stephen Muldrow USAFLM Re Dr. Asad Qamar May-12-2017Neil GillespieNo ratings yet
- Chapter 5 - Counselling Skills: The GP As An Effective CounsellorDocument19 pagesChapter 5 - Counselling Skills: The GP As An Effective Counsellorprofarmah6150100% (2)
- Rubella: Congenital Clinically Significant Congenital MalformationsDocument8 pagesRubella: Congenital Clinically Significant Congenital MalformationsAlexandraNo ratings yet
- Evaluation of Meat Quality and Carcass Characteristics of Broiler Chickens As Affected by Feed Withdrawal With Electrolytes Added To WaterDocument8 pagesEvaluation of Meat Quality and Carcass Characteristics of Broiler Chickens As Affected by Feed Withdrawal With Electrolytes Added To WaterInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- PRO Measures - Shoulder and Upper ExtremityDocument27 pagesPRO Measures - Shoulder and Upper ExtremityGonzalo QuiñonesNo ratings yet
- Rumah Sakit Bhakti MuliaDocument3 pagesRumah Sakit Bhakti MuliaSarachanda SallyNo ratings yet