You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Sterlization of Water Using Bleaching Powder PDFDocument20 pagesSterlization of Water Using Bleaching Powder PDFradha krishnanNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- SASMO 2020 Grade 6 + SolutionDocument24 pagesSASMO 2020 Grade 6 + SolutionBentley Leopold Halim94% (18)
- Serial Number AutoCAD 2014Document5 pagesSerial Number AutoCAD 2014Punith Ky67% (9)
- ASME Fatigue Life CurvesDocument3 pagesASME Fatigue Life CurvesnamasralNo ratings yet
- Advisor Webcast Exadata Disk Management and Troubleshotting Tips FinalDocument84 pagesAdvisor Webcast Exadata Disk Management and Troubleshotting Tips FinalethenhuntNo ratings yet
- Seguridad Electrica 4Document28 pagesSeguridad Electrica 4salo081018No ratings yet
- 9 EndometriosisDocument475 pages9 EndometriosisDelviDeavia100% (2)
- FirmcusbDocument123 pagesFirmcusbAndry1975No ratings yet
- Dpu 6055Document54 pagesDpu 6055Daniel PricopNo ratings yet
- The Effect of Sugar on Behavior or Cognition in Children: A Meta-analysisDocument5 pagesThe Effect of Sugar on Behavior or Cognition in Children: A Meta-analysisIqra AnugerahNo ratings yet
- Counselling Who 2013 PDFDocument244 pagesCounselling Who 2013 PDFericasftNo ratings yet
- UterotonicAgent FactSheet ShieldsDocument2 pagesUterotonicAgent FactSheet Shieldsmanleyj5305No ratings yet
- Management of Antiphospholipid SyndromeDocument18 pagesManagement of Antiphospholipid SyndromeIqra AnugerahNo ratings yet
- 10.1016 j.jmwh.2006.07.005Document8 pages10.1016 j.jmwh.2006.07.005Iqra AnugerahNo ratings yet
- PSP MPC Topic-06Document13 pagesPSP MPC Topic-06Iqra Anugerah100% (1)
- Single-dose treatment as effective as standard therapy for vaginal dischargeDocument10 pagesSingle-dose treatment as effective as standard therapy for vaginal dischargeIqra AnugerahNo ratings yet
- Pregnancy infections inadequately managed by syndromic approachDocument10 pagesPregnancy infections inadequately managed by syndromic approachIqra AnugerahNo ratings yet
- Jepm 2 118Document5 pagesJepm 2 118Joni MokodoNo ratings yet
- Diagnostic Frozen SectionDocument8 pagesDiagnostic Frozen SectionIqra AnugerahNo ratings yet
- Co 620Document4 pagesCo 620Iqra AnugerahNo ratings yet
- Management Stress Urinary IncontinenceDocument8 pagesManagement Stress Urinary IncontinenceIqra AnugerahNo ratings yet
- IUD TranslocationDocument3 pagesIUD TranslocationIqra AnugerahNo ratings yet
- ICS IUGA Joint Report On The Terminology For Female Pelvic Organ Prolapse POPDocument32 pagesICS IUGA Joint Report On The Terminology For Female Pelvic Organ Prolapse POPIqra AnugerahNo ratings yet
- Conversion Laparoscopy To Laparotomy For Total HysterectomyDocument11 pagesConversion Laparoscopy To Laparotomy For Total HysterectomyIqra AnugerahNo ratings yet
- Faecal Incontinence: Useful Contacts Further InformationDocument2 pagesFaecal Incontinence: Useful Contacts Further InformationIqra AnugerahNo ratings yet
- 22 - ESHRE Guideline On Endometriosis 2013 PDFDocument97 pages22 - ESHRE Guideline On Endometriosis 2013 PDFsaryindrianyNo ratings yet
- Pi Is 0090825816303638Document2 pagesPi Is 0090825816303638Iqra AnugerahNo ratings yet
- Complication of Laparoscopic SurgeryDocument5 pagesComplication of Laparoscopic SurgeryIqra AnugerahNo ratings yet
- Management Stress Urinary IncontinenceDocument8 pagesManagement Stress Urinary IncontinenceIqra AnugerahNo ratings yet
- Laparoscopic Removal of Translocated Retroperitoneal IUD: K.K. Roy, N. Banerjee, A. SinhaDocument3 pagesLaparoscopic Removal of Translocated Retroperitoneal IUD: K.K. Roy, N. Banerjee, A. SinhaIqra AnugerahNo ratings yet
- Bruner Tran - 2013 - Medical Management of Endometriosis - Emerging Evidence Linking Inflammation To Disease PathophysiologyDocument18 pagesBruner Tran - 2013 - Medical Management of Endometriosis - Emerging Evidence Linking Inflammation To Disease PathophysiologyIqra AnugerahNo ratings yet
- Technical Update On Physiology Amniotic FluidDocument7 pagesTechnical Update On Physiology Amniotic FluidIqra AnugerahNo ratings yet
- Endometrial Hyperplasia Management G40 v2Document7 pagesEndometrial Hyperplasia Management G40 v2Iqra AnugerahNo ratings yet
- Conversion Laparoscopy To Laparotomy For Total HysterectomyDocument11 pagesConversion Laparoscopy To Laparotomy For Total HysterectomyIqra AnugerahNo ratings yet
- Brown - 2014 - Endometriosis - An Overview of Cochrane Reviews (Review)Document44 pagesBrown - 2014 - Endometriosis - An Overview of Cochrane Reviews (Review)Iqra AnugerahNo ratings yet
- Guideline On The Management of Anogenita WartsDocument9 pagesGuideline On The Management of Anogenita WartsIqra AnugerahNo ratings yet
- Comparison of Three Different Hemostatic Devices in Laparoscopic MyomectomyDocument5 pagesComparison of Three Different Hemostatic Devices in Laparoscopic MyomectomyIqra AnugerahNo ratings yet
- Physical symbol system hypothesis: An overviewDocument5 pagesPhysical symbol system hypothesis: An overviewKostasBaliotisNo ratings yet
- The Importance of Calculators in Math ClassDocument6 pagesThe Importance of Calculators in Math Classchloe shanice bordiosNo ratings yet
- Holiday Assignment XDocument2 pagesHoliday Assignment XMonis ShaikhNo ratings yet
- Design of Bulk CarrierDocument7 pagesDesign of Bulk CarrierhoangductuanNo ratings yet
- 8 Bevel ProtractorsDocument4 pages8 Bevel Protractorssomu_amuNo ratings yet
- PSE YRC1000micro 00Document25 pagesPSE YRC1000micro 00LiemNo ratings yet
- Power Max India PVT LTD Extra Work Done at VMW Shed WorksDocument4 pagesPower Max India PVT LTD Extra Work Done at VMW Shed WorksparthaNo ratings yet
- Analyze Sales Performance with Key FiguresDocument192 pagesAnalyze Sales Performance with Key Figurespanirbanonline3426No ratings yet
- DefinitionsHypothesesPosterior Analytics (Landor)Document12 pagesDefinitionsHypothesesPosterior Analytics (Landor)Daniel Rojas UNo ratings yet
- AtmegaDocument22 pagesAtmegaMUKILANNo ratings yet
- DBA Roles and ResponsibilitiesDocument2 pagesDBA Roles and ResponsibilitiesMahesh Babu Sri100% (2)
- The Road Beyond 5G: A Vision and Insight of The Key TechnologiesDocument7 pagesThe Road Beyond 5G: A Vision and Insight of The Key TechnologiesSaurav SarkarNo ratings yet
- Amd690gm-M2 1219Document34 pagesAmd690gm-M2 1219rmartins_239474No ratings yet
- S4M Service ManualDocument522 pagesS4M Service ManualRafał Krzysztof Kowalski100% (1)
- NFRC 200-2010Document45 pagesNFRC 200-2010reynolds534100% (1)
- Pages 296-298 Module 6 ReviewDocument4 pagesPages 296-298 Module 6 Reviewapi-332361871No ratings yet
- MCQ Metrology (CCCM & CCCT) PDFDocument21 pagesMCQ Metrology (CCCM & CCCT) PDFSahil Gauhar67% (3)
- Mos PDFDocument194 pagesMos PDFChoon Ewe LimNo ratings yet
- NMNR5104 Research MethodologyDocument2 pagesNMNR5104 Research MethodologynadiaNo ratings yet
- GH Chap 78 - Insulin, Glucagon and DMDocument16 pagesGH Chap 78 - Insulin, Glucagon and DMShellz2428No ratings yet
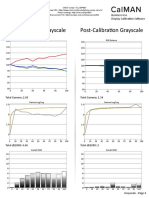
- TCL 55P607 CNET Review Calibration ResultsDocument3 pagesTCL 55P607 CNET Review Calibration ResultsDavid KatzmaierNo ratings yet
- Ecen 326 - Lab 2 ReportDocument7 pagesEcen 326 - Lab 2 Reportapi-241454978No ratings yet