You might also like
- tratamiento con AINESDocument6 pagestratamiento con AINESCarol Chávez MedinaNo ratings yet
- Miwa 2016Document13 pagesMiwa 2016asri nurul ismiNo ratings yet
- Ghost AuthorDocument13 pagesGhost AuthorjbahalkehNo ratings yet
- Digestive PDFDocument10 pagesDigestive PDFRahmat AgungNo ratings yet
- Alimentary TractDocument8 pagesAlimentary Tractgrace liwantoNo ratings yet
- A Candidate Probiotic With Unfavourable Effects in Subjects With Irritable Bowel Syndrome: A Randomised Controlled TrialDocument7 pagesA Candidate Probiotic With Unfavourable Effects in Subjects With Irritable Bowel Syndrome: A Randomised Controlled Trialdolo2000No ratings yet
- Factors Affecting The Prevalence of Gastro-Oesophageal Reflux in Childhood Corrosive Oesophageal StricturesDocument6 pagesFactors Affecting The Prevalence of Gastro-Oesophageal Reflux in Childhood Corrosive Oesophageal StricturesAlinaRellyyNo ratings yet
- Iihyuyu6756e54tw5w3553w5et6yfug5757 Jgut75Document6 pagesIihyuyu6756e54tw5w3553w5et6yfug5757 Jgut75RIBNo ratings yet
- Troxipide vs. Rabeprazole in The Treatment of GastritisDocument8 pagesTroxipide vs. Rabeprazole in The Treatment of GastritisZuventusHealthcareNo ratings yet
- VBBVBVBVBVBVBVBBVDocument17 pagesVBBVBVBVBVBVBVBBVAYUE ZONE PRATITISNo ratings yet
- Gastric mucus thickness chronic gastritis fucoidanDocument6 pagesGastric mucus thickness chronic gastritis fucoidanmelz_mocaNo ratings yet
- A Prospective Observational Study of Prescribing Patterns in Peptic Ulcer DiseaseDocument40 pagesA Prospective Observational Study of Prescribing Patterns in Peptic Ulcer DiseaseGeet MaanNo ratings yet
- OutDocument15 pagesOutIulia IonelaNo ratings yet
- Ibuprofen, A Potential Cause of Acute Hemorrhagic Gastritis in Children - A Case ReportDocument4 pagesIbuprofen, A Potential Cause of Acute Hemorrhagic Gastritis in Children - A Case ReportOmegawati PramudyaNo ratings yet
- Pathophysiology/Pathogenesis of PUDDocument4 pagesPathophysiology/Pathogenesis of PUDvan_cristianoNo ratings yet
- Rebamipide and Pantoprazole Combination in NSAIDs-Gastropathy TreatmentDocument5 pagesRebamipide and Pantoprazole Combination in NSAIDs-Gastropathy TreatmentSabrina JonesNo ratings yet
- Claus R. Riedl - Hyaluronan Treatment of Interstitial Cystitispainful Bladder SyDocument5 pagesClaus R. Riedl - Hyaluronan Treatment of Interstitial Cystitispainful Bladder SyMed TouhamiNo ratings yet
- GI Side Effects of NSAIDSDocument11 pagesGI Side Effects of NSAIDSSree BanNo ratings yet
- The Effect of Non-Steroidal Anti-Inflammatory Drugs On Severity of Acute Pancreatitis and Pancreatic NecrosisDocument4 pagesThe Effect of Non-Steroidal Anti-Inflammatory Drugs On Severity of Acute Pancreatitis and Pancreatic NecrosisAracelyAcostaNo ratings yet
- 1756 0500 6 116Document6 pages1756 0500 6 116Muhammad AsrizalNo ratings yet
- Randomized Controlled Trial of Transoral IncisionlessDocument13 pagesRandomized Controlled Trial of Transoral IncisionlessResidentes CirugiaNo ratings yet
- Lansoprazole For The Prevention of Recurrences of Ulcer Complications From Long-Term Low-Dose Aspirin UseDocument6 pagesLansoprazole For The Prevention of Recurrences of Ulcer Complications From Long-Term Low-Dose Aspirin UseAmalia NandiaNo ratings yet
- Hemorragia Digestiva Alta: Manejo Actual Diagnostico y TratmientoDocument2 pagesHemorragia Digestiva Alta: Manejo Actual Diagnostico y TratmientoLuis Rafael Suárez U.No ratings yet
- Tofacitinib As Induction and Maintenance Therapy For Ulcerative ColitisDocument14 pagesTofacitinib As Induction and Maintenance Therapy For Ulcerative Colitismichal ben meronNo ratings yet
- NSAID Colon UlcersDocument5 pagesNSAID Colon UlcersFrederic IkkiNo ratings yet
- Hansen2005 2Document10 pagesHansen2005 2charmainegoNo ratings yet
- HTTP WWW - Sciencedirect.com Science Ob MImg& Imagekey B6WP1-4HK01J7-7-1& Cdi 6977& User 8187385& OrigDocument4 pagesHTTP WWW - Sciencedirect.com Science Ob MImg& Imagekey B6WP1-4HK01J7-7-1& Cdi 6977& User 8187385& OrigBimalKrishnaNo ratings yet
- 2011 A Randomized Controlled Trial of Laparoscopic Nissen Fundoplication Versus PPIs For The Treatment of Patients With GERDDocument8 pages2011 A Randomized Controlled Trial of Laparoscopic Nissen Fundoplication Versus PPIs For The Treatment of Patients With GERDResidentes Cirugia Udea 2016No ratings yet
- Vonoprazan 10 MG DailyDocument5 pagesVonoprazan 10 MG DailySanjay NavaleNo ratings yet
- Endoscopic Evaluation of Aceclofenac Gastrointestinal SafetyDocument11 pagesEndoscopic Evaluation of Aceclofenac Gastrointestinal SafetyMartin MoranNo ratings yet
- Impact of Percutaneous Endoscopic Gastrostomy On Gastroesophageal Reflux and Gastric Emptying in Pediatric Patients GER and Gastric Emptying After PEGDocument5 pagesImpact of Percutaneous Endoscopic Gastrostomy On Gastroesophageal Reflux and Gastric Emptying in Pediatric Patients GER and Gastric Emptying After PEGInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Use of Inhaled NaceDocument7 pagesThe Use of Inhaled NaceYondi Piter PapulungNo ratings yet
- NSAID and drug-induced peptic ulcer diseaseDocument4 pagesNSAID and drug-induced peptic ulcer diseasewindanurmaliya3356No ratings yet
- 5short Term Efficacy of Potassium Competitive Acid Blocker Following Gastric Endoscopic Submucosal Dissection A Propensity Score AnalysisDocument10 pages5short Term Efficacy of Potassium Competitive Acid Blocker Following Gastric Endoscopic Submucosal Dissection A Propensity Score AnalysisVicNo ratings yet
- Clinical Outcomes of Esophagogastroduodenoscopy In.27Document6 pagesClinical Outcomes of Esophagogastroduodenoscopy In.27Agung KaryawinaraNo ratings yet
- H pylori treatment in functional dyspepsia resistant to acid inhibitorsDocument7 pagesH pylori treatment in functional dyspepsia resistant to acid inhibitorsyostiNo ratings yet
- 1 s2.0 S246812532300208X MainDocument14 pages1 s2.0 S246812532300208X MainPiyush malikNo ratings yet
- RESEARCH - GERD-Q Score DLBS2411-hiresDocument8 pagesRESEARCH - GERD-Q Score DLBS2411-hiresNanangNo ratings yet
- Ceju 66 00246Document4 pagesCeju 66 00246Àlex MataNo ratings yet
- Savarino 2016Document6 pagesSavarino 2016Aulia Bahtiar RahmanNo ratings yet
- Comparison of Omeprazole and Ranitidine For Stress Ulcer ProphylaxisDocument5 pagesComparison of Omeprazole and Ranitidine For Stress Ulcer ProphylaxisAngelica Hurtado CollanteNo ratings yet
- Comparison of Octreotide and Hyoscine in Controlling Gastrointestinal Symptoms Due To Malignant Inoperable Bowel ObstructionDocument4 pagesComparison of Octreotide and Hyoscine in Controlling Gastrointestinal Symptoms Due To Malignant Inoperable Bowel ObstructionThiago GomesNo ratings yet
- Electrical Stimulation Therapy of The Lower Esophageal Sphincter Is Successful in Treating GERD - Long-Term 3-Year ResultsDocument7 pagesElectrical Stimulation Therapy of The Lower Esophageal Sphincter Is Successful in Treating GERD - Long-Term 3-Year Resultsdavid.stuart.thompsonNo ratings yet
- ReemDocument13 pagesReemSAYED ZAKINo ratings yet
- Long Acting Octreotide For The Treatment and Symptomatic Relief of Bowel Obstruction in Advanced Ovarian CancerDocument7 pagesLong Acting Octreotide For The Treatment and Symptomatic Relief of Bowel Obstruction in Advanced Ovarian CancerThiago GomesNo ratings yet
- New guidelines acute diarrheaDocument4 pagesNew guidelines acute diarrheaOvilia Mutiara SantikaNo ratings yet
- Systematic Review: Antacids, H - Receptor Antagonists, Prokinetics, Bismuth and Sucralfate Therapy For Non-Ulcer DyspepsiaDocument13 pagesSystematic Review: Antacids, H - Receptor Antagonists, Prokinetics, Bismuth and Sucralfate Therapy For Non-Ulcer DyspepsiaAaquib AmirNo ratings yet
- Palliative Stenting With or Without Radiotherapy For Inoperable Esophageal CarcinomaDocument7 pagesPalliative Stenting With or Without Radiotherapy For Inoperable Esophageal CarcinomaBella StevannyNo ratings yet
- InTech-Pharmacological Therapy For Recurrent Obscure Gastrointestinal BleedingDocument13 pagesInTech-Pharmacological Therapy For Recurrent Obscure Gastrointestinal BleedingPETERNo ratings yet
- The Search For Disease-Modifying Agents in Decompensated Cirrhosis: From Drug Repurposing To Drug DiscoveryDocument17 pagesThe Search For Disease-Modifying Agents in Decompensated Cirrhosis: From Drug Repurposing To Drug Discoverymuhamad deniansyahNo ratings yet
- MelissaDocument9 pagesMelissaDemi-America Vega LaraNo ratings yet
- Shinozaki Japan VanoprazanDocument9 pagesShinozaki Japan Vanoprazansahama2508No ratings yet
- Art 1 HT3Document3 pagesArt 1 HT3Glenda MaríaNo ratings yet
- Adverse Event Chloroquine 1Document8 pagesAdverse Event Chloroquine 1Ingrid KoutioNo ratings yet
- Complications of Proton Pump Inhibitor Therapy 2017Document14 pagesComplications of Proton Pump Inhibitor Therapy 2017Ingrid Miroslava Reyes DiazNo ratings yet
- Comprehensive Management of ArdDocument12 pagesComprehensive Management of ArdParamitha DonaNo ratings yet
- Jurnal 3 Fater 2Document8 pagesJurnal 3 Fater 2ANDIANY CAHYANTY TAHIRNo ratings yet
- Double Blind Randomized Placebo-Controlled Trial To Evaluate The Efficacy and Safety of Short-Course Low Dose Oral Prednisolone in Pityriasis RoseaDocument10 pagesDouble Blind Randomized Placebo-Controlled Trial To Evaluate The Efficacy and Safety of Short-Course Low Dose Oral Prednisolone in Pityriasis RoseaSalsabila Munirah AmirNo ratings yet
- A Study of Preoperative Predictive Factors of Strangulation in Acute Small Intestinal ObstructionDocument6 pagesA Study of Preoperative Predictive Factors of Strangulation in Acute Small Intestinal ObstructionSantosh BabuNo ratings yet
- Comparative Study of Atorvastatin and RosuvastatinDocument8 pagesComparative Study of Atorvastatin and RosuvastatinDewi nur thohidahNo ratings yet
- JurnalDocument9 pagesJurnalYanuar Ahsan OfficialNo ratings yet
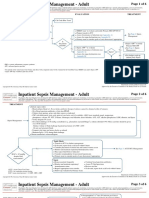
- Inpatient Sepsis Management - Adult: Page 1 of 6Document6 pagesInpatient Sepsis Management - Adult: Page 1 of 6Dewi nur thohidahNo ratings yet
- Comparative Study of Atorvastatin and RosuvastatinDocument8 pagesComparative Study of Atorvastatin and RosuvastatinDewi nur thohidahNo ratings yet
- 1 PBDocument11 pages1 PBDewi nur thohidahNo ratings yet
- Chronic Kidney Disease Stage V: (Laporan Kasus)Document5 pagesChronic Kidney Disease Stage V: (Laporan Kasus)Alif Fabri OktanoNo ratings yet
- Advpub Ess14061Document10 pagesAdvpub Ess14061Dewi nur thohidahNo ratings yet
- At Some ConcentrationsDocument7 pagesAt Some ConcentrationsDewi nur thohidahNo ratings yet
- Extraction and Evaluation of Piperine From Piper Nigrum Linn.Document6 pagesExtraction and Evaluation of Piperine From Piper Nigrum Linn.Dewi nur thohidahNo ratings yet
- Anti-Inflammatory Activity of Medicinal Plants A ReviewDocument10 pagesAnti-Inflammatory Activity of Medicinal Plants A ReviewDewi nur thohidahNo ratings yet
- Chronic Kidney Disease Stage V: (Laporan Kasus)Document5 pagesChronic Kidney Disease Stage V: (Laporan Kasus)Alif Fabri OktanoNo ratings yet
- Antimicrobial Activity of SpicesDocument55 pagesAntimicrobial Activity of SpicesDewi nur thohidahNo ratings yet
- 3023 6565 2 PB PDFDocument5 pages3023 6565 2 PB PDFpopy AinunNo ratings yet
- Recognize and Treatment of Digitalis Intoxication: Case ReportDocument6 pagesRecognize and Treatment of Digitalis Intoxication: Case ReportKilroy Vincent SterlingNo ratings yet
- Https FarterDocument1 pageHttps FarterDewi nur thohidahNo ratings yet
- INJEKSI LARUTAN SODIUM DIKLOFENAKDocument35 pagesINJEKSI LARUTAN SODIUM DIKLOFENAKDewi nur thohidahNo ratings yet
- Peningkatan Kualitas Lada Putih Dengan Kombinasi LamaDocument9 pagesPeningkatan Kualitas Lada Putih Dengan Kombinasi LamaDewi nur thohidahNo ratings yet
- Parametric Optimization of Microwave Reflux Extraction of Spice Oleoresin From White Pepper (Piper Nigrum)Document8 pagesParametric Optimization of Microwave Reflux Extraction of Spice Oleoresin From White Pepper (Piper Nigrum)Dewi nur thohidahNo ratings yet
- Extraction and Evaluation of Piperine From Piper Nigrum Linn.Document6 pagesExtraction and Evaluation of Piperine From Piper Nigrum Linn.Dewi nur thohidahNo ratings yet
- Parametric Optimization of Microwave Reflux Extraction of Spice Oleoresin From White Pepper (Piper Nigrum)Document8 pagesParametric Optimization of Microwave Reflux Extraction of Spice Oleoresin From White Pepper (Piper Nigrum)Dewi nur thohidahNo ratings yet
- Antimicrobial Activity of SpicesDocument55 pagesAntimicrobial Activity of SpicesDewi nur thohidahNo ratings yet
- Antimicrobial Activity of SpicesDocument55 pagesAntimicrobial Activity of SpicesDewi nur thohidahNo ratings yet
- Antimicrobial Herb and Spice Compounds in FoodDocument20 pagesAntimicrobial Herb and Spice Compounds in FoodPrabowo SuryaningtyasNo ratings yet
- Anti-Obesity Efficacy of Nanoemulsion OleoresinDocument10 pagesAnti-Obesity Efficacy of Nanoemulsion OleoresinDewi nur thohidahNo ratings yet
- ParkinsonDocument9 pagesParkinsonDaniel OctavianusNo ratings yet
- Nutmeg's (Myristica Fragrans Houtt) Oleoresin Effect of Heating To Chemical Compositions and Antifungal PropertiesDocument11 pagesNutmeg's (Myristica Fragrans Houtt) Oleoresin Effect of Heating To Chemical Compositions and Antifungal PropertiesDewi nur thohidahNo ratings yet
- HFHS CKD V6Document76 pagesHFHS CKD V6medicalNo ratings yet
- A Review On Potential Families of Anti-Inflammatory ActivityDocument15 pagesA Review On Potential Families of Anti-Inflammatory ActivityDewi nur thohidahNo ratings yet
- Chronic Kidney Disease Stage V: (Laporan Kasus)Document5 pagesChronic Kidney Disease Stage V: (Laporan Kasus)Alif Fabri OktanoNo ratings yet
- Anti-Inflammatory Activity of Medicinal Plants A ReviewDocument10 pagesAnti-Inflammatory Activity of Medicinal Plants A ReviewDewi nur thohidahNo ratings yet
- Diagnosis and Management of Placenta PreviaDocument6 pagesDiagnosis and Management of Placenta PreviaNoveno Semestre FmuaqNo ratings yet
- CholedocholithiasisDocument9 pagesCholedocholithiasisOsiithaa CañaszNo ratings yet
- Medscape Hypovolemic ShockDocument14 pagesMedscape Hypovolemic ShockSarah Ovinitha100% (1)
- Types of Medical Equipment, Rooms and Departments in HospitalDocument22 pagesTypes of Medical Equipment, Rooms and Departments in HospitalAfriza EffendiNo ratings yet
- False UnicornDocument3 pagesFalse UnicornNutrimakeNo ratings yet
- PCODDocument76 pagesPCODShreyance Parakh100% (1)
- Arju 5Document3 pagesArju 5arjumardi azrahNo ratings yet
- Water For Injections BP: What Is in This Leaflet?Document2 pagesWater For Injections BP: What Is in This Leaflet?Mohamed OmerNo ratings yet
- Potential Long-Term Side Effects of Exposure To ChemoDocument21 pagesPotential Long-Term Side Effects of Exposure To ChemoMichael BubleNo ratings yet
- Uterine Rupture: South Australian Perinatal Practice GuidelineDocument8 pagesUterine Rupture: South Australian Perinatal Practice GuidelineMaiNisNo ratings yet
- 13 - Surgical InfectionsDocument26 pages13 - Surgical InfectionsEma KhalilNo ratings yet
- Note Making and Note TakingDocument33 pagesNote Making and Note TakingManisha SalikarNo ratings yet
- Final exam questions on obstetrics and gynaecologyDocument1 pageFinal exam questions on obstetrics and gynaecologySlashy HeugotNo ratings yet
- Rita Alcaraz: Clinical Experience and SkillsDocument1 pageRita Alcaraz: Clinical Experience and Skillsapi-398600648No ratings yet
- Ama Journal of EthicsDocument5 pagesAma Journal of EthicsJonathan JoseNo ratings yet
- Outcome of Teenage PregnancyDocument5 pagesOutcome of Teenage PregnancyKN DumpNo ratings yet
- Antibiotic in Obstetric and GynecologyDocument36 pagesAntibiotic in Obstetric and GynecologyDrAbdi YusufNo ratings yet
- High-Risk Pregnancy Premature Rupture of Membranes (PROM)Document3 pagesHigh-Risk Pregnancy Premature Rupture of Membranes (PROM)elimcangcoNo ratings yet
- LR Partograph FormDocument1 pageLR Partograph FormJILL ANGELES50% (2)
- Medical Record WikipediaDocument4 pagesMedical Record WikipediaRisma KurniaNo ratings yet
- What is a phobia? Types, causes and treatmentDocument3 pagesWhat is a phobia? Types, causes and treatmentLaura La Novia ImaginariaNo ratings yet
- The Pharmacist Guide To Implementing Pharmaceutical Care PDFDocument502 pagesThe Pharmacist Guide To Implementing Pharmaceutical Care PDFLuis SosaNo ratings yet
- Diagnostic Centers ListDocument38 pagesDiagnostic Centers ListSaurav BansalNo ratings yet
- Red Alert - Infant Vaginal BleedingDocument5 pagesRed Alert - Infant Vaginal BleedingmonicamoniccNo ratings yet
- Obstetric Emergencies PDFDocument15 pagesObstetric Emergencies PDFEdi BackyNo ratings yet
- Considerations On The Use of Neonatal and Pediatric ResuscitationDocument15 pagesConsiderations On The Use of Neonatal and Pediatric ResuscitationrsmitrahuadaNo ratings yet
- Fetal Lung MaturityDocument17 pagesFetal Lung MaturityAkbarNovan100% (1)
- Clinical Questions of Upper LimbDocument5 pagesClinical Questions of Upper LimbAyushiNo ratings yet
- NCM109 RLE 1st Term ReviewerDocument40 pagesNCM109 RLE 1st Term ReviewerCarelle Faith Serrano AsuncionNo ratings yet
- VawpregnancyDocument2 pagesVawpregnancyOkto 'Andri' SaputraNo ratings yet