You might also like
- LED-Based Photoacoustic Imaging: From Bench to BedsideFrom EverandLED-Based Photoacoustic Imaging: From Bench to BedsideMithun Kuniyil Ajith SinghNo ratings yet
- Photo Accoustic ImagineDocument7 pagesPhoto Accoustic ImagineArpan MannaNo ratings yet
- Low-Noise, High-Gain Transimpedance Amplifier Integrated With Siapd For Low-Intensity Near-Infrared Light DetectionDocument13 pagesLow-Noise, High-Gain Transimpedance Amplifier Integrated With Siapd For Low-Intensity Near-Infrared Light Detectionantoine.sayerNo ratings yet
- Clinical Use and Research Applications of Heidelberg Retinal Angiography and Spectral-Domain Optical Coherence Tomography - A ReviewDocument14 pagesClinical Use and Research Applications of Heidelberg Retinal Angiography and Spectral-Domain Optical Coherence Tomography - A ReviewMashhoor AlfayezNo ratings yet
- photonics-08-00127-v2Document13 pagesphotonics-08-00127-v2oprea.traian01No ratings yet
- Broadband Picometer-Scale Resolution On-Chip Spectrometer With Reconfigurable PhotonicsDocument10 pagesBroadband Picometer-Scale Resolution On-Chip Spectrometer With Reconfigurable PhotonicsarashmokhtariNo ratings yet
- Clinical Photoacoustic Imaging.... AttiaDocument18 pagesClinical Photoacoustic Imaging.... AttiaChadiIbrahimNo ratings yet
- 10 1002@mp 16199Document19 pages10 1002@mp 16199Nima SalianiNo ratings yet
- Status and Prospects of Digital Detector Technology For CR and DRDocument7 pagesStatus and Prospects of Digital Detector Technology For CR and DRBisnis KitaNo ratings yet
- A Practical Guide To Photoacoustic Tomography in The Life SciencesDocument12 pagesA Practical Guide To Photoacoustic Tomography in The Life SciencesyuyiipNo ratings yet
- kVp Estimate Comparison Between Three InstrumentsDocument5 pageskVp Estimate Comparison Between Three InstrumentsvictorNo ratings yet
- Medical Physics - 2021 - Lee - Medical X Band Linear Accelerator For High Precision RadiotherapyDocument16 pagesMedical Physics - 2021 - Lee - Medical X Band Linear Accelerator For High Precision RadiotherapyNima SalianiNo ratings yet
- Energy Response of Imaging Plates to Standard Beta SourcesDocument8 pagesEnergy Response of Imaging Plates to Standard Beta SourcesJoko WidodoNo ratings yet
- 1 s2.0 S1687850721003289 MainDocument10 pages1 s2.0 S1687850721003289 Mainsouhaila soulNo ratings yet
- Bartzsch 2017 Phys. Med. Biol. 62 8600Document17 pagesBartzsch 2017 Phys. Med. Biol. 62 8600Piotr JankowskiNo ratings yet
- A Novel Photodiode For Reflectance Pulse PDFDocument4 pagesA Novel Photodiode For Reflectance Pulse PDFSàkâtã ÁbéŕàNo ratings yet
- Darambara 2002Document6 pagesDarambara 2002nasreddine boutaghaneNo ratings yet
- MRM 85 495Document11 pagesMRM 85 495natiNo ratings yet
- (2019) Flexible, Printable Soft-X-Ray Detectors Based On All-Inorganic Perovskite Quantum DotsDocument8 pages(2019) Flexible, Printable Soft-X-Ray Detectors Based On All-Inorganic Perovskite Quantum DotsCarlos PereiraNo ratings yet
- New laser offers advanced technology for retina proceduresDocument3 pagesNew laser offers advanced technology for retina proceduresmunchen88No ratings yet
- Bio-Inspired Polarization Imaging Sensors: From Circuits and Optics To Signal Processing Algorithms and Biomedical ApplicationsDocument16 pagesBio-Inspired Polarization Imaging Sensors: From Circuits and Optics To Signal Processing Algorithms and Biomedical ApplicationsJaya SwaroopNo ratings yet
- 2012 - Ostertag, Merz, Kessler - Multimodal Spatially Resolved Near-Field Scattering and Absorption Spectroscopy - Nanoscale Imaging, SeDocument10 pages2012 - Ostertag, Merz, Kessler - Multimodal Spatially Resolved Near-Field Scattering and Absorption Spectroscopy - Nanoscale Imaging, SeClaudio BiaginiNo ratings yet
- 247 2006 Article 208-1Document10 pages247 2006 Article 208-1NavnetNo ratings yet
- Deep Learning Enables Superior Photoacoustic Imaging at Ultralow Laser DosagesDocument11 pagesDeep Learning Enables Superior Photoacoustic Imaging at Ultralow Laser DosagesElizabeth EspitiaNo ratings yet
- Alternative X-Ray Filters For An Intra-Oral Digital Radiographic SystemDocument6 pagesAlternative X-Ray Filters For An Intra-Oral Digital Radiographic SystemXUB xNo ratings yet
- Correlation of Image Quality Parameters With Tube Voltage in X Ray Dark Field Chest Radiography: A Phantom StudyDocument8 pagesCorrelation of Image Quality Parameters With Tube Voltage in X Ray Dark Field Chest Radiography: A Phantom Studyhandikajati kusumaNo ratings yet
- Digital Radiography ReviewDocument4 pagesDigital Radiography ReviewEka JuliantaraNo ratings yet
- RSI WengkungDocument10 pagesRSI Wengkung164616444No ratings yet
- Development of An Active Intravascular MR Device With An Optical Transmission SystemDocument5 pagesDevelopment of An Active Intravascular MR Device With An Optical Transmission SystemasifnewazuccNo ratings yet
- Photovoltaic Restoration of Sight With High Visual Acuity: ArticlesDocument10 pagesPhotovoltaic Restoration of Sight With High Visual Acuity: ArticleswatsonNo ratings yet
- Master Thesis Optical Coherence TomographyDocument6 pagesMaster Thesis Optical Coherence Tomographydebbirchrochester100% (2)
- Optoelectronic Retinal ProsthesisDocument13 pagesOptoelectronic Retinal ProsthesisSpoorthy HUNo ratings yet
- Model QP & Answers - v2Document14 pagesModel QP & Answers - v2dr.yuvarajvelusamy2No ratings yet
- SeleniumDocument11 pagesSeleniumkoszt.igorNo ratings yet
- Development and in Vivo Performance Evaluation of 1060-MHz Band Impulse-Radio-Based Transceiver For Deep Implantation Having 10 MbpsDocument9 pagesDevelopment and in Vivo Performance Evaluation of 1060-MHz Band Impulse-Radio-Based Transceiver For Deep Implantation Having 10 MbpsYoga VyshnaviNo ratings yet
- Definition of Terms Physical LaserDocument17 pagesDefinition of Terms Physical LaserEllahnae VelasquezNo ratings yet
- App Medical Laser ServiceDocument3 pagesApp Medical Laser ServiceMIKENo ratings yet
- Ijpbs 4272 PDFDocument11 pagesIjpbs 4272 PDFVenkatramanNo ratings yet
- Biomedical Photoacoustic ImagingDocument30 pagesBiomedical Photoacoustic ImagingGuy CohenNo ratings yet
- A Comparison of 18 Different X-Ray Detectors Currently UsedDocument5 pagesA Comparison of 18 Different X-Ray Detectors Currently UsedpnogrlNo ratings yet
- Weiland EMBS 2005Document3 pagesWeiland EMBS 2005Kumar PrabhatNo ratings yet
- Acousto-Optic Catheter Tracking Sensor For Interventional MRI ProceduresDocument7 pagesAcousto-Optic Catheter Tracking Sensor For Interventional MRI ProceduresasifnewazuccNo ratings yet
- ALT - 2018 Book of AbstractsDocument184 pagesALT - 2018 Book of Abstractspopovichnatasha2211No ratings yet
- Digital MamografiaDocument10 pagesDigital MamografiaElias SebelenNo ratings yet
- Lasers For Medical: CO2/Excimer/Semiconductor Diodes/OPSL/Fiber ComponentsDocument12 pagesLasers For Medical: CO2/Excimer/Semiconductor Diodes/OPSL/Fiber ComponentsMostafaOkpelbabNo ratings yet
- 2013-Organic Light Detectors - Photodiodes and PhototransistorsDocument29 pages2013-Organic Light Detectors - Photodiodes and PhototransistorsNguyen Minh Vuong TT. TNTHNo ratings yet
- Esplen 2022 Phys. Med. Biol. 67 105003Document25 pagesEsplen 2022 Phys. Med. Biol. 67 105003souhaila soulNo ratings yet
- Radiodiagnosis Thesis TopicsDocument8 pagesRadiodiagnosis Thesis Topicsjmvnqiikd100% (2)
- Optical Coherence TomographyDocument36 pagesOptical Coherence TomographyLaura NitaNo ratings yet
- Radiation Doses of Indirect and Direct Digital CepDocument5 pagesRadiation Doses of Indirect and Direct Digital CepdentureNo ratings yet
- Tutorial On Photoacoustic Microscopy and Computed TomographyDocument9 pagesTutorial On Photoacoustic Microscopy and Computed TomographyadiNo ratings yet
- Flexible and Broadband Colloidal Quantum Dots Photodiode Array For Pixel-Level X-Ray To Near-Infrared Image FusionDocument9 pagesFlexible and Broadband Colloidal Quantum Dots Photodiode Array For Pixel-Level X-Ray To Near-Infrared Image Fusion18877544451No ratings yet
- Performance of A Low Gain Avalanche Detector in ADocument12 pagesPerformance of A Low Gain Avalanche Detector in AAbdellatif TalbiNo ratings yet
- Polymer Infrared Proximity Sensor ArrayDocument6 pagesPolymer Infrared Proximity Sensor ArrayWhiteCrossesNo ratings yet
- Shimadzu UV-3600 Plus UV-VIS-NIR Spectrophotometer ReportDocument5 pagesShimadzu UV-3600 Plus UV-VIS-NIR Spectrophotometer ReportWaqar ShehbazNo ratings yet
- Published Article 3Document5 pagesPublished Article 3Bharathi RajaNo ratings yet
- Ultra-Wideband Confocal Microwave Imaging For Brain Tumor DetectionDocument8 pagesUltra-Wideband Confocal Microwave Imaging For Brain Tumor DetectionAwais QureshiNo ratings yet
- Femto Laser in OphthalmologyDocument11 pagesFemto Laser in Ophthalmologylycan007No ratings yet
- Msot For CancerDocument12 pagesMsot For CancerChadiIbrahimNo ratings yet
- In Vivo: 910nm Femtosecond Nd-Doped Fiber Laser For Two-Photon Microscopic ImagingDocument6 pagesIn Vivo: 910nm Femtosecond Nd-Doped Fiber Laser For Two-Photon Microscopic ImagingLiveta MiliauskaitėNo ratings yet
- Bernard 2017 Changing Target Temp From 33 To 36Document5 pagesBernard 2017 Changing Target Temp From 33 To 36Steven BrownNo ratings yet
- Bradley 2018 Oi 180199Document11 pagesBradley 2018 Oi 180199Steven BrownNo ratings yet
- Mortality in Patients With OHCA - HACORE RegistryDocument10 pagesMortality in Patients With OHCA - HACORE RegistrySteven BrownNo ratings yet
- DW General Price List Esu 191219 NQ MedicalDocument2 pagesDW General Price List Esu 191219 NQ MedicalSteven BrownNo ratings yet
- Salter 2018 - Changes in Temperature Management of Cardiac Arrest Patients Following Publication of The Target Temperature Management TrialDocument9 pagesSalter 2018 - Changes in Temperature Management of Cardiac Arrest Patients Following Publication of The Target Temperature Management TrialSteven BrownNo ratings yet
- Operational Amplifier (Op-Amp) (Cont.) : Electronic Devices For Biomedical DesignDocument24 pagesOperational Amplifier (Op-Amp) (Cont.) : Electronic Devices For Biomedical DesignSteven BrownNo ratings yet
- Electrosurgical Unit Dt-300S/400S Specification: No. Factor Daiwha Product SpecificationDocument1 pageElectrosurgical Unit Dt-300S/400S Specification: No. Factor Daiwha Product SpecificationSteven BrownNo ratings yet
- Khera ROCDocument11 pagesKhera ROCSteven BrownNo ratings yet
- 9 2012 Deqs Chap3a1Document113 pages9 2012 Deqs Chap3a1Steven BrownNo ratings yet
- 2019 ICEM PCC and TTM Training Course Program Including Invitation LetterDocument3 pages2019 ICEM PCC and TTM Training Course Program Including Invitation LetterSteven BrownNo ratings yet
- Electrosurgical Unit Dt-300S/400S Specification: No. Factor Daiwha Product SpecificationDocument1 pageElectrosurgical Unit Dt-300S/400S Specification: No. Factor Daiwha Product SpecificationSteven BrownNo ratings yet
- Dong Sahn Jenix Co., LTD.: SpecificationDocument1 pageDong Sahn Jenix Co., LTD.: SpecificationSteven BrownNo ratings yet
- Key Final RevisionDocument2 pagesKey Final RevisionSteven BrownNo ratings yet
- DW General Price List Esu 191219 NQ MedicalDocument2 pagesDW General Price List Esu 191219 NQ MedicalSteven BrownNo ratings yet
- Chris Bumstead PPL PDFDocument8 pagesChris Bumstead PPL PDFBrandon Foley94% (17)
- Charles Glass The Godfather of Bodybuilding First ChapterDocument8 pagesCharles Glass The Godfather of Bodybuilding First Chapterbelal rashad67% (21)
- Chris Jones Push Pull LegsDocument26 pagesChris Jones Push Pull Legshaathabaitun30288% (24)
- Hospital Bed Specs & FeaturesDocument2 pagesHospital Bed Specs & FeaturesSteven BrownNo ratings yet
- Infusion Pump Ds-3000 Specification: No. Factor Daiwha Product SpecificationDocument1 pageInfusion Pump Ds-3000 Specification: No. Factor Daiwha Product SpecificationSteven BrownNo ratings yet
- Electrosurgical Unit Dt-300S/400S Specification: No. Factor Daiwha Product SpecificationDocument1 pageElectrosurgical Unit Dt-300S/400S Specification: No. Factor Daiwha Product SpecificationSteven BrownNo ratings yet
- BMK CO.,LTD instrument cabinet specsDocument1 pageBMK CO.,LTD instrument cabinet specsSteven BrownNo ratings yet
- Jejoong Medical Co.,Ltd.: SpecificationDocument1 pageJejoong Medical Co.,Ltd.: SpecificationSteven BrownNo ratings yet
- Hospital Bed Specs & FeaturesDocument2 pagesHospital Bed Specs & FeaturesSteven BrownNo ratings yet
- Health Care Korea Co.: SpecificationDocument1 pageHealth Care Korea Co.: SpecificationSteven BrownNo ratings yet
- Hospital Bed Specs & FeaturesDocument2 pagesHospital Bed Specs & FeaturesSteven BrownNo ratings yet
- BMK TC7545 2SDocument1 pageBMK TC7545 2SSteven BrownNo ratings yet
- BMK DC6545 4SDocument1 pageBMK DC6545 4SSteven BrownNo ratings yet
- BMK Ivs2Document1 pageBMK Ivs2Steven BrownNo ratings yet
- BMK WHCDocument1 pageBMK WHCSteven BrownNo ratings yet
- BMK FDCDocument1 pageBMK FDCSteven BrownNo ratings yet
- Economic Case for Immobilizing EnzymesDocument25 pagesEconomic Case for Immobilizing EnzymesNikki ChauhanNo ratings yet
- Emerging Foodborne Enteric Bacterial Pathogens: A ReviewDocument11 pagesEmerging Foodborne Enteric Bacterial Pathogens: A ReviewAngelica Alejandra De La Torre AnayaNo ratings yet
- Comparing Food with Comparative AdjectivesDocument4 pagesComparing Food with Comparative AdjectivesLuisito GonzalezNo ratings yet
- Tutorial Sheet 4Document2 pagesTutorial Sheet 4Syed YousufuddinNo ratings yet
- FD2000 DatasheetDocument2 pagesFD2000 DatasheetIvan MihajlovicNo ratings yet
- Deliver VALUE and RENEWABLE FUTUREDocument30 pagesDeliver VALUE and RENEWABLE FUTUREAlexandru SuciuNo ratings yet
- Mitsubishi Galant 4g63 Engine Repair ManualDocument29 pagesMitsubishi Galant 4g63 Engine Repair ManualMoaed Kanbar100% (1)
- Indian Pharmacopiea 2007Document73 pagesIndian Pharmacopiea 2007Deepak ShahNo ratings yet
- Main Receiving Station PDFDocument8 pagesMain Receiving Station PDFPrakash Kumar0% (1)
- Conveying Water Distribution SEODocument90 pagesConveying Water Distribution SEOmichelghanemNo ratings yet
- Agriculture Class-8Document67 pagesAgriculture Class-8Sahej100% (2)
- Lubricants: Chapter - 5 Lubricants and LubricationDocument5 pagesLubricants: Chapter - 5 Lubricants and LubricationMalaika AzeemNo ratings yet
- Research PresentationDocument13 pagesResearch Presentationapi-252252011No ratings yet
- Automated Hematology Cell Counters 12-09-2023Document161 pagesAutomated Hematology Cell Counters 12-09-2023Tom JohnathanNo ratings yet
- Herbal MedicineDocument38 pagesHerbal MedicineBurei KouNo ratings yet
- Fuente As-IDocument4 pagesFuente As-IadalaviNo ratings yet
- Yoga & Diet To Prevent DepressionDocument5 pagesYoga & Diet To Prevent DepressionDietician Mrunmayee DixitNo ratings yet
- Dutch FarmDocument104 pagesDutch Farmdoc_abdullahNo ratings yet
- SimmonsDocument12 pagesSimmonsGürelBaltalıNo ratings yet
- Population Ecology: Aecc-I +3 1 YearDocument32 pagesPopulation Ecology: Aecc-I +3 1 YearAnita kumari SahuNo ratings yet
- Substrates P400 enDocument111 pagesSubstrates P400 enLince WijoyoNo ratings yet
- NBME 22 OfflineDocument200 pagesNBME 22 OfflineGautham Kanagala86% (14)
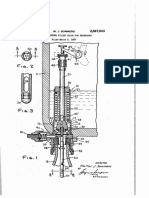
- Counter-pressure filler valve for beveragesDocument3 pagesCounter-pressure filler valve for beveragesbimalishaNo ratings yet
- By Kerri Rivera, Kimberly Mcdaniel and Daniel Bender: Healing The Symptoms Known As Autism Second EditionDocument24 pagesBy Kerri Rivera, Kimberly Mcdaniel and Daniel Bender: Healing The Symptoms Known As Autism Second EditionMarilen De Leon EbradaNo ratings yet
- Experiment 1 Marble Race Virtual Science Lab Chem 2Document4 pagesExperiment 1 Marble Race Virtual Science Lab Chem 2Oribe, Narciso A.100% (1)
- BW Mc2 XWHM y Na ManualDocument23 pagesBW Mc2 XWHM y Na ManualSatyasrinivas PulavarthiNo ratings yet
- OTC Drug ListDocument7 pagesOTC Drug ListHong Diem100% (1)
- Understanding the Relationship Between Place and HealthDocument14 pagesUnderstanding the Relationship Between Place and HealtheNo ratings yet
- Amul India Case Study: Product Portfolio and SWOT AnalysisDocument10 pagesAmul India Case Study: Product Portfolio and SWOT AnalysisShruti NagmoteNo ratings yet
- Sakshijain75.Final ProDocument46 pagesSakshijain75.Final ProOm AherNo ratings yet
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- Wayfinding: The Science and Mystery of How Humans Navigate the WorldFrom EverandWayfinding: The Science and Mystery of How Humans Navigate the WorldRating: 4.5 out of 5 stars4.5/5 (18)
- Alex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessFrom EverandAlex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessNo ratings yet
- Fire Season: Field Notes from a Wilderness LookoutFrom EverandFire Season: Field Notes from a Wilderness LookoutRating: 4 out of 5 stars4/5 (142)
- Dark Matter and the Dinosaurs: The Astounding Interconnectedness of the UniverseFrom EverandDark Matter and the Dinosaurs: The Astounding Interconnectedness of the UniverseRating: 3.5 out of 5 stars3.5/5 (69)
- The Other End of the Leash: Why We Do What We Do Around DogsFrom EverandThe Other End of the Leash: Why We Do What We Do Around DogsRating: 5 out of 5 stars5/5 (64)
- World of Wonders: In Praise of Fireflies, Whale Sharks, and Other AstonishmentsFrom EverandWorld of Wonders: In Praise of Fireflies, Whale Sharks, and Other AstonishmentsRating: 4 out of 5 stars4/5 (222)
- The Ancestor's Tale: A Pilgrimage to the Dawn of EvolutionFrom EverandThe Ancestor's Tale: A Pilgrimage to the Dawn of EvolutionRating: 4 out of 5 stars4/5 (811)
- Why Fish Don't Exist: A Story of Loss, Love, and the Hidden Order of LifeFrom EverandWhy Fish Don't Exist: A Story of Loss, Love, and the Hidden Order of LifeRating: 4.5 out of 5 stars4.5/5 (699)
- Come Back, Como: Winning the Heart of a Reluctant DogFrom EverandCome Back, Como: Winning the Heart of a Reluctant DogRating: 3.5 out of 5 stars3.5/5 (10)
- The Lives of Bees: The Untold Story of the Honey Bee in the WildFrom EverandThe Lives of Bees: The Untold Story of the Honey Bee in the WildRating: 4.5 out of 5 stars4.5/5 (44)
- The Revolutionary Genius of Plants: A New Understanding of Plant Intelligence and BehaviorFrom EverandThe Revolutionary Genius of Plants: A New Understanding of Plant Intelligence and BehaviorRating: 4.5 out of 5 stars4.5/5 (137)
- When You Find Out the World Is Against You: And Other Funny Memories About Awful MomentsFrom EverandWhen You Find Out the World Is Against You: And Other Funny Memories About Awful MomentsRating: 3.5 out of 5 stars3.5/5 (13)
- Spoiled Rotten America: Outrages of Everyday LifeFrom EverandSpoiled Rotten America: Outrages of Everyday LifeRating: 3 out of 5 stars3/5 (19)
- The Hidden Life of Trees: What They Feel, How They CommunicateFrom EverandThe Hidden Life of Trees: What They Feel, How They CommunicateRating: 4 out of 5 stars4/5 (1002)
- The Secret Life of Lobsters: How Fishermen and Scientists Are Unraveling the Mysteries of Our Favorite CrustaceanFrom EverandThe Secret Life of Lobsters: How Fishermen and Scientists Are Unraveling the Mysteries of Our Favorite CrustaceanNo ratings yet
- Gathering Moss: A Natural and Cultural History of MossesFrom EverandGathering Moss: A Natural and Cultural History of MossesRating: 4.5 out of 5 stars4.5/5 (349)