You might also like
- Neuro Case StudyDocument24 pagesNeuro Case StudyJenyl BajadoNo ratings yet
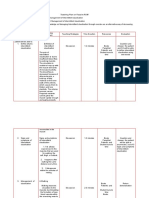
- Teaching Plan MeeeeeDocument6 pagesTeaching Plan MeeeeeJenyl BajadoNo ratings yet
- A Case Study of Urinary Tract Infection 2Document23 pagesA Case Study of Urinary Tract Infection 2Jenyl BajadoNo ratings yet
- Drug Dosage Action/Indication Side Effect Contraindications Nursing Responsibility AmpicillinDocument1 pageDrug Dosage Action/Indication Side Effect Contraindications Nursing Responsibility AmpicillinJenyl BajadoNo ratings yet
- Application of Demographic Transition On Health Program PlanningDocument5 pagesApplication of Demographic Transition On Health Program PlanningJenyl BajadoNo ratings yet
- CDC IiiDocument5 pagesCDC IiiJenyl BajadoNo ratings yet
- Dosage & Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing Responsibility Rivotril ClassificationDocument5 pagesDosage & Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing Responsibility Rivotril ClassificationJenyl BajadoNo ratings yet
- Postpartum ExerciseDocument14 pagesPostpartum ExerciseJenyl BajadoNo ratings yet
- Drug Dosage Action/Indication Side Effect Contraindications Nursing Responsibility AmpicillinDocument1 pageDrug Dosage Action/Indication Side Effect Contraindications Nursing Responsibility AmpicillinJenyl BajadoNo ratings yet
- Life Cycles of Common ParasitesDocument15 pagesLife Cycles of Common ParasitesJenyl BajadoNo ratings yet
- Lipids or FatsDocument5 pagesLipids or FatsJenyl BajadoNo ratings yet
- Nutrition During Childhood and AdolescentDocument40 pagesNutrition During Childhood and AdolescentJenyl BajadoNo ratings yet
- Toddler and FamilyDocument28 pagesToddler and FamilyJenyl BajadoNo ratings yet
- Promoting Breastfeeding: Physiology, Benefits & ManagementDocument24 pagesPromoting Breastfeeding: Physiology, Benefits & ManagementJenyl Bajado100% (1)
- IV FluidsDocument7 pagesIV FluidsJenyl BajadoNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Research Paper For AbortionDocument10 pagesResearch Paper For AbortionMarevisha Vidfather75% (4)
- Wto Unit-2Document19 pagesWto Unit-2Anwar KhanNo ratings yet
- A Case of Eclectic Family TherapyDocument88 pagesA Case of Eclectic Family Therapygun gorNo ratings yet
- Municipal Ordinance No. 05-2008Document5 pagesMunicipal Ordinance No. 05-2008SBGuinobatan100% (2)
- List of Pakistani Government Ministries and DivisionsDocument2 pagesList of Pakistani Government Ministries and DivisionsbasitaleeNo ratings yet
- Dental Restorative Digital Workflow: Digital Smile Design From Aesthetic To Function PDFDocument12 pagesDental Restorative Digital Workflow: Digital Smile Design From Aesthetic To Function PDFCamilo GuerreroNo ratings yet
- A Deep Learning Approach To Antibiotic DiscoveryDocument29 pagesA Deep Learning Approach To Antibiotic DiscoveryDeepika ChhabraNo ratings yet
- Heavy Water Board RecruitmentDocument7 pagesHeavy Water Board RecruitmentramavarshnyNo ratings yet
- Getting HSE Right A Guide For BP Managers 2001Document62 pagesGetting HSE Right A Guide For BP Managers 2001Muhammad Labib Subhani0% (1)
- Swollen Feet During PregnancyDocument2 pagesSwollen Feet During PregnancyDede YasminNo ratings yet
- Mbaeri Accuracy of Prader OrchidometerDocument4 pagesMbaeri Accuracy of Prader OrchidometerChikezie OnwukweNo ratings yet
- Co General InformationDocument13 pagesCo General InformationAndianto IndrawanNo ratings yet
- MudreDocument10 pagesMudrejezebelvertNo ratings yet
- Gurr2011-Probleme Psihologice Dupa Atac CerebralDocument9 pagesGurr2011-Probleme Psihologice Dupa Atac CerebralPaulNo ratings yet
- Hypertension Drugs Cheat Sheet: by ViaDocument3 pagesHypertension Drugs Cheat Sheet: by ViaGulzaib KhokharNo ratings yet
- Competitive Tennis For Young PlayersDocument146 pagesCompetitive Tennis For Young PlayersTuzos100% (1)
- Cough and ColdsDocument3 pagesCough and ColdsKarl-Ren Lacanilao100% (1)
- Case Control Study For MedicDocument41 pagesCase Control Study For Medicnunu ahmedNo ratings yet
- Tingkat KesadaranDocument16 pagesTingkat KesadaranShinta NurjanahNo ratings yet
- Ba - Bacterial Identification Lab WorksheetDocument12 pagesBa - Bacterial Identification Lab WorksheetFay SNo ratings yet
- FoundationDocument10 pagesFoundationBardoNo ratings yet
- MCQ BankDocument23 pagesMCQ Bankdrmed100% (3)
- Report On Legal Medicine PowerpointDocument31 pagesReport On Legal Medicine PowerpointEdwin VillaNo ratings yet
- Barriers To Bystander CPR in Deprived Communities: Findings From A Qualitative StudyDocument11 pagesBarriers To Bystander CPR in Deprived Communities: Findings From A Qualitative Studygevowo3277No ratings yet
- Acute Tracheobronchitis Causes, Symptoms, TreatmentDocument2 pagesAcute Tracheobronchitis Causes, Symptoms, TreatmentNicole Shannon CariñoNo ratings yet
- Cyclone Shelter Construction Maintenance and Management Policy 2011Document21 pagesCyclone Shelter Construction Maintenance and Management Policy 2011MAHABUBUR RAHAMANNo ratings yet
- Tailored Health Plans Table of CoverDocument22 pagesTailored Health Plans Table of CoverAneesh PrabhakaranNo ratings yet
- Part A Reading Task Playground Injuries Playground Surface MaterialDocument8 pagesPart A Reading Task Playground Injuries Playground Surface MaterialMitra NabizadehNo ratings yet
- Labcorp: Patient ReportDocument4 pagesLabcorp: Patient ReportAsad PrinceNo ratings yet
- Calculate The Max Doses of Local Anesthesia in DentistryDocument13 pagesCalculate The Max Doses of Local Anesthesia in DentistryYasser MagramiNo ratings yet