You might also like
- A Cough That Won't Go Away Evaluation and Treatment in 2 PatientsDocument7 pagesA Cough That Won't Go Away Evaluation and Treatment in 2 Patientshossein kasiriNo ratings yet
- CDU Care Plan. UTIDocument7 pagesCDU Care Plan. UTImutiso mutieNo ratings yet
- Irritable Bowel Syndrome: Heal Your Gut Naturally in 90 Days!From EverandIrritable Bowel Syndrome: Heal Your Gut Naturally in 90 Days!No ratings yet
- Case Study in Vesicovaginal FistulaDocument14 pagesCase Study in Vesicovaginal FistulaIvory100% (4)
- Ulcerative Colitis, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandUlcerative Colitis, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Share 'Useful Signal Markers - PDF'Document20 pagesShare 'Useful Signal Markers - PDF'Loredana DobreaNo ratings yet
- Elevated Deoxycholic Acid and Idiopathic Recurrent Acute PancreatitisDocument3 pagesElevated Deoxycholic Acid and Idiopathic Recurrent Acute PancreatitisMaria LimaNo ratings yet
- Cholera Case StudyDocument44 pagesCholera Case StudyKrisianne Mae Lorenzo Francisco100% (3)
- Functional Heartburn. An Underrecognized Cause of PPI-refractory Symptoms 2019Document8 pagesFunctional Heartburn. An Underrecognized Cause of PPI-refractory Symptoms 2019Ricardo Robles AlfaroNo ratings yet
- Acute Gastroenteritis (Age)Document37 pagesAcute Gastroenteritis (Age)Jay Ar SantiagoNo ratings yet
- Diarrhea and dehydration in man and daughter returning from MexicoDocument18 pagesDiarrhea and dehydration in man and daughter returning from Mexicowira rila zulmaNo ratings yet
- Anaphylactic Shock GROUP 2 RLEDocument83 pagesAnaphylactic Shock GROUP 2 RLEJanine Mae MacaraigNo ratings yet
- Worksheets - Isbar Week 4 x2Document3 pagesWorksheets - Isbar Week 4 x2api-631170779No ratings yet
- I. Biographic DataDocument12 pagesI. Biographic DataYsrael AlcantaraNo ratings yet
- Ibuprofen and Chronic Pyloric StrictureDocument8 pagesIbuprofen and Chronic Pyloric StricturejuliaNo ratings yet
- Useful Signal MarkersDocument20 pagesUseful Signal MarkersMar ClrNo ratings yet
- NCM 112a Case Study-GphDocument6 pagesNCM 112a Case Study-GphbabesNo ratings yet
- Management of DiarrheaDocument12 pagesManagement of DiarrheaHammo Ez AldienNo ratings yet
- Case Study 39-Year-Old Women Diagnosed As Solitary Rectal Ulcer SyndromeDocument5 pagesCase Study 39-Year-Old Women Diagnosed As Solitary Rectal Ulcer SyndromeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Chorioamnionitis Drug StudyDocument9 pagesChorioamnionitis Drug Studyjunard2580100% (1)
- (Mayo Clinic Proceedings, Jan 2022) - 75 Year Old Woman With Abdominal Pain and ConstipationDocument5 pages(Mayo Clinic Proceedings, Jan 2022) - 75 Year Old Woman With Abdominal Pain and ConstipationNigelyulNo ratings yet
- Irritable Bowel SyndromeDocument8 pagesIrritable Bowel Syndromea_chiekaNo ratings yet
- I Patient Assessment Data BaseDocument12 pagesI Patient Assessment Data BaseJanice_Fernand_1603No ratings yet
- Case Presentation On Ectopic Pregnancy ... NewDocument13 pagesCase Presentation On Ectopic Pregnancy ... NewPabhat Kumar91% (32)
- Colon's Role in Chronic ArthritisDocument5 pagesColon's Role in Chronic ArthritisIG0% (1)
- Cadisal MW 1ST Week RequiementsDocument36 pagesCadisal MW 1ST Week RequiementsJonathan GonzalesNo ratings yet
- Pub Med 1Document4 pagesPub Med 1Kaouther KiouaneNo ratings yet
- Acute Appendicitis - CSDocument29 pagesAcute Appendicitis - CSMASIINo ratings yet
- Rafa - Patient AssesmentDocument8 pagesRafa - Patient AssesmentRafa HassanNo ratings yet
- Chronic Diarrhea PDFDocument5 pagesChronic Diarrhea PDFnaryNo ratings yet
- Posting ElectiveDocument7 pagesPosting ElectiveThulasi tootsieNo ratings yet
- Abdominal TB Causing Intestinal ObstructionDocument10 pagesAbdominal TB Causing Intestinal ObstructionCleoanne GallegosNo ratings yet
- A Diagnostic Problem and Family AssessmentDocument7 pagesA Diagnostic Problem and Family AssessmentLandy de la CruzNo ratings yet
- Recurrent Severe Vomitting Due To Hyperthyroidsm: Case ReportDocument13 pagesRecurrent Severe Vomitting Due To Hyperthyroidsm: Case ReportRia sandita wulandariNo ratings yet
- Genitourinary TuberculosisDocument16 pagesGenitourinary Tuberculosisdokter.kicikNo ratings yet
- Bonifacio Case Study GPHDocument6 pagesBonifacio Case Study GPHbabesNo ratings yet
- Ectopic Pregnancy Case StudyDocument16 pagesEctopic Pregnancy Case StudyMacMacNo ratings yet
- Morning Report - PyelonephritisDocument54 pagesMorning Report - PyelonephritisjonNo ratings yet
- Nejmcp 2114026Document10 pagesNejmcp 2114026Cristina Adriana PopaNo ratings yet
- Khoory 2Document2 pagesKhoory 2Salamah KhooryNo ratings yet
- Diagnstico Diferencial de Vmitos PDFDocument9 pagesDiagnstico Diferencial de Vmitos PDFLeoberto Batista Pereira SobrinhoNo ratings yet
- Nutrition Issues in GastroenterologyDocument10 pagesNutrition Issues in GastroenterologyjinniNo ratings yet
- Intestinal Malrotation in Neonates With Nonbilious Emesis: Perinatal/Neonatal Case PresentationDocument3 pagesIntestinal Malrotation in Neonates With Nonbilious Emesis: Perinatal/Neonatal Case PresentationSaurav SultaniaNo ratings yet
- CMC-Preterm LaborDocument11 pagesCMC-Preterm LaborRalph AlbertoNo ratings yet
- 4th Year Write Up 2 - Int. MedDocument11 pages4th Year Write Up 2 - Int. MedLoges TobyNo ratings yet
- Case Study Tumor LysisDocument28 pagesCase Study Tumor Lysisapi-653850652No ratings yet
- Augmenten (Amoxicillin Clavulan)Document2 pagesAugmenten (Amoxicillin Clavulan)Adrianne BazoNo ratings yet
- Nejmcp 2114026Document10 pagesNejmcp 2114026Engin AltınkayaNo ratings yet
- Jurnal IndoDocument21 pagesJurnal IndoAnonymous ce3S6XFdwUNo ratings yet
- Acute Glomerulonephritis - CSDocument31 pagesAcute Glomerulonephritis - CSMASIINo ratings yet
- Case Presentation 2Document11 pagesCase Presentation 2Angel Jonele ManongsongNo ratings yet
- REFERENSIDocument7 pagesREFERENSIDesyRosaNo ratings yet
- New Diagnostic Test For Dogs With Chronic Gastrointestinal SignsDocument2 pagesNew Diagnostic Test For Dogs With Chronic Gastrointestinal SignsvetthamilNo ratings yet
- Pre-Eclampsia Secondary to Uncontrolled Hypertension: A Case StudyDocument21 pagesPre-Eclampsia Secondary to Uncontrolled Hypertension: A Case StudyRhose Angel AzurNo ratings yet
- Next Step Advanced Medical Coding and Auditing 2017 2018 Edition 1st Edition Buck Test BankDocument25 pagesNext Step Advanced Medical Coding and Auditing 2017 2018 Edition 1st Edition Buck Test BankAllisonPowersrjqo100% (48)
- AppendicitisDocument11 pagesAppendicitisayuniNo ratings yet
- Cough As The Presenting Symptom of Pancreatic AdenocarcinomaDocument6 pagesCough As The Presenting Symptom of Pancreatic AdenocarcinomaJanibel BaezNo ratings yet
- Causes and Effect of Drug AddictionDocument3 pagesCauses and Effect of Drug AddictionEdmund HalleyNo ratings yet
- Influenza in Brazil: Surveillance Pathways: Regional ReviewDocument11 pagesInfluenza in Brazil: Surveillance Pathways: Regional ReviewThaís Nunes dos AnjosNo ratings yet
- ASOTDocument4 pagesASOTemperors_nestNo ratings yet
- Decline of Feudalism Student NotebookDocument8 pagesDecline of Feudalism Student Notebookapi-2334644940% (2)
- Dermatologic DiseaseDocument31 pagesDermatologic Diseaseعبدالسلام الأسمرNo ratings yet
- Trans Pulmopatho ColoredDocument8 pagesTrans Pulmopatho Colored2012No ratings yet
- Schmitt NF JumpDocument1 pageSchmitt NF JumpKim PalmieroNo ratings yet
- Presented By:-Himanshu Dev DMLT VI TH Sem. VMMC & SJHDocument55 pagesPresented By:-Himanshu Dev DMLT VI TH Sem. VMMC & SJHKailash Nagar100% (1)
- Medical Biology 3Document42 pagesMedical Biology 3Malik MohamedNo ratings yet
- Briefing Note: Antimicrobial Resistance: An Emerging Water, Sanitation and Hygiene IssueDocument16 pagesBriefing Note: Antimicrobial Resistance: An Emerging Water, Sanitation and Hygiene IssueBoni MagtibayNo ratings yet
- Ap Biology CH 19 Reading GuideDocument4 pagesAp Biology CH 19 Reading Guideapi-293174360No ratings yet
- Event 201Document5 pagesEvent 201Pandu DhioNo ratings yet
- Medical MycologyDocument94 pagesMedical MycologyNozomiNo ratings yet
- Urinalysis Lab ReportDocument3 pagesUrinalysis Lab Reportapi-194371846100% (2)
- EMQ Samples MicrobiologyDocument5 pagesEMQ Samples MicrobiologyHugh JacobsNo ratings yet
- International Rice Research Newsletter Vol.5 No.1Document24 pagesInternational Rice Research Newsletter Vol.5 No.1ccquintosNo ratings yet
- Majalah Popular Mechanics USA - October 2016Document121 pagesMajalah Popular Mechanics USA - October 2016Iswan PuteraNo ratings yet
- November 9, 2011 Emily Gogarty Chris Sokoloff Queen's University MECH478Document20 pagesNovember 9, 2011 Emily Gogarty Chris Sokoloff Queen's University MECH478Chris SoksNo ratings yet
- Blood Cells and The Hematopoetic SystemDocument53 pagesBlood Cells and The Hematopoetic SystemMeet RandhawaNo ratings yet
- Erythroderma: Review of A Potentially Life-Threatening DermatosisDocument12 pagesErythroderma: Review of A Potentially Life-Threatening DermatosisAdatyaStevaniP.PutuhenaNo ratings yet
- Points to Remember: Classification SystemsDocument10 pagesPoints to Remember: Classification SystemsANo ratings yet
- Animal InoculationDocument10 pagesAnimal InoculationAnumol LoranceNo ratings yet
- JCR Article PDFDocument3 pagesJCR Article PDFSai KalyanNo ratings yet
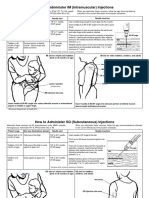
- Im SQ Admin PDFDocument2 pagesIm SQ Admin PDFAlvin JjNo ratings yet
- Dental Caries Student ProjectDocument6 pagesDental Caries Student Projectapi-3705762No ratings yet
- Laboratory Manual Mic341 (Latest)Document25 pagesLaboratory Manual Mic341 (Latest)Iman Fatihah0% (1)
- Tonsillitis Anatomy, Causes, Symptoms and TreatmentDocument29 pagesTonsillitis Anatomy, Causes, Symptoms and TreatmentDwi Utari PratiwiNo ratings yet
- Recurrent Herpes LabialisDocument25 pagesRecurrent Herpes LabialisGarry B GunawanNo ratings yet
- NCP To NG PneumoniaDocument3 pagesNCP To NG PneumoniaGlenn Asuncion PagaduanNo ratings yet
- Neonatal SepsisDocument22 pagesNeonatal Sepsisjake1014100% (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)