You might also like
- WHO RHR 18.05 EngDocument7 pagesWHO RHR 18.05 EngCarlos CastroNo ratings yet
- Handout - ADocument13 pagesHandout - AMadhu UpadhyayNo ratings yet
- Anti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Document27 pagesAnti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Widy StefannyNo ratings yet
- Nicotine Replacement Therapy in Preg & LactationDocument3 pagesNicotine Replacement Therapy in Preg & LactationYwagar YwagarNo ratings yet
- National Drug Policy 2013Document15 pagesNational Drug Policy 2013sahidNo ratings yet
- Immunization Clinic Report PDFDocument9 pagesImmunization Clinic Report PDFprabha krishnanNo ratings yet
- Improve Maternal and Child Health with BEmOC ProgramsDocument6 pagesImprove Maternal and Child Health with BEmOC ProgramsMenard VelascoNo ratings yet
- Amplify The Learning (Ob) Week #4 - 1: Vidon, Aubrey Rose A. April 18, 2020 BSN 2Y2-2Document2 pagesAmplify The Learning (Ob) Week #4 - 1: Vidon, Aubrey Rose A. April 18, 2020 BSN 2Y2-2AriaNo ratings yet
- Indian Academy of Pediatrics (IAP) Recommended Immunization Schedule For Children Aged 0 Through 18 Years - India, 2014 and Updates On ImmunizationDocument16 pagesIndian Academy of Pediatrics (IAP) Recommended Immunization Schedule For Children Aged 0 Through 18 Years - India, 2014 and Updates On Immunizationkrishna615No ratings yet
- Summary of Neurodisability WorkshopDocument6 pagesSummary of Neurodisability WorkshopYogeshRavalNo ratings yet
- 5.tuberculosis in PregnancyDocument36 pages5.tuberculosis in PregnancyMuhammad Ahmad SyammakhNo ratings yet
- Study of Effectiveness of DMPA in Postpartum and Postabortal PeriodDocument5 pagesStudy of Effectiveness of DMPA in Postpartum and Postabortal PeriodInternational Organization of Scientific Research (IOSR)No ratings yet
- WHO Recommendations On Antenatal Care For A Positive Pregnancy Experience: SummaryDocument10 pagesWHO Recommendations On Antenatal Care For A Positive Pregnancy Experience: SummaryShalim BagusNo ratings yet
- Guideline WHO PIT Page 21-38 Important NotesDocument3 pagesGuideline WHO PIT Page 21-38 Important NotesRizki Akbar SentosaNo ratings yet
- Paper Qualitative Plos One MalariaDocument12 pagesPaper Qualitative Plos One Malariaamiruddin_jamaluddinNo ratings yet
- Indian Academy of Pediatrics (IAP) Recommended Immunization Schedule 2013Document14 pagesIndian Academy of Pediatrics (IAP) Recommended Immunization Schedule 2013Mahesh ShankarNo ratings yet
- Anx 130395 enDocument48 pagesAnx 130395 enMehdiNo ratings yet
- Contraception and FertilityDocument11 pagesContraception and FertilityWil LesterNo ratings yet
- New PMTCT ProtocolDocument30 pagesNew PMTCT ProtocolNti JepoNo ratings yet
- Answer Key Midwifery 1 Final Term ExaminationDocument6 pagesAnswer Key Midwifery 1 Final Term Examinationgladz25No ratings yet
- Evidence Based Contraceptive ManagementDocument11 pagesEvidence Based Contraceptive ManagementPatrick BayuNo ratings yet
- tb-section-8-anti-tuberculosis-drugsDocument4 pagestb-section-8-anti-tuberculosis-drugsparkviewinternending2023No ratings yet
- Unang Yakap: Why Moms Should Include It in Their Birth PlansDocument3 pagesUnang Yakap: Why Moms Should Include It in Their Birth PlansTyron ChuaNo ratings yet
- Dosing Interval Between Mifepristone and Misoprostol in Second and Third Trimester TerminationDocument5 pagesDosing Interval Between Mifepristone and Misoprostol in Second and Third Trimester TerminationWILMER HUANGANo ratings yet
- Clinical management of tuberculosis with a focus on gastrointestinal TBDocument5 pagesClinical management of tuberculosis with a focus on gastrointestinal TBparmar jalpabenNo ratings yet
- Why Postpartum Family PlanningDocument20 pagesWhy Postpartum Family PlanningAyana FiromsaNo ratings yet
- Frequently Asked Questions On Use of Medicines in Pregnancy (2) Vol.12 No.6 2006Document7 pagesFrequently Asked Questions On Use of Medicines in Pregnancy (2) Vol.12 No.6 2006Agung IstiawanNo ratings yet
- UTIDocument4 pagesUTIVagabond RabbyNo ratings yet
- TB Guideline TreatmentDocument14 pagesTB Guideline TreatmentNovii NoviiNo ratings yet
- Pumonary Tuberculosis in Pregnancy PALLAVI PptDocument42 pagesPumonary Tuberculosis in Pregnancy PALLAVI PptJyothsna DeepNo ratings yet
- Chapter 3 EincDocument31 pagesChapter 3 EincHaru YukiNo ratings yet
- Obat Anti Tuberkulosis Pada Ibu HamilDocument27 pagesObat Anti Tuberkulosis Pada Ibu HamilIful SaifullahNo ratings yet
- Immunization-WPS OfficeDocument3 pagesImmunization-WPS OfficeFranc'isco ChidiebereNo ratings yet
- Annex I Summary of Product CharacteristicsDocument83 pagesAnnex I Summary of Product CharacteristicsKarthik YadaNo ratings yet
- Preventive Obstetrics SeminarDocument25 pagesPreventive Obstetrics SeminarAnju MargaretNo ratings yet
- Expectant Management On Preterm Pregnancy With Preeclampsia: A Scoping ReviewDocument7 pagesExpectant Management On Preterm Pregnancy With Preeclampsia: A Scoping Reviewunisa magisterNo ratings yet
- Active Management of 3RD Stage of LaborDocument7 pagesActive Management of 3RD Stage of LaborFarheen khanNo ratings yet
- DR Bernadette Daelmans WHO PresentationDocument20 pagesDR Bernadette Daelmans WHO PresentationMaternal and Child Survival Program (MCSP)No ratings yet
- Eng 50 65Document16 pagesEng 50 65DESI SCORPINASARINo ratings yet
- Nursing Intervention Reduces Nausea During PregnancyDocument12 pagesNursing Intervention Reduces Nausea During PregnancyNaga AdfenNo ratings yet
- Everything You Need to Know About Injectable ContraceptivesDocument97 pagesEverything You Need to Know About Injectable Contraceptivesganapa247No ratings yet
- Maternity Ati RemediationDocument2 pagesMaternity Ati Remediationcse100% (1)
- Up To Date. Tuberculosis TreatmentDocument55 pagesUp To Date. Tuberculosis TreatmentGuardito PequeñoNo ratings yet
- Vaccine and ImmunizationDocument54 pagesVaccine and ImmunizationSivaNo ratings yet
- L The Importance of Emergency ContraceptionDocument20 pagesL The Importance of Emergency ContraceptionAsma BegumNo ratings yet
- WHO Immunization Schedule ChildrenDocument9 pagesWHO Immunization Schedule Childrenashchua21No ratings yet
- 2015 Article 794Document9 pages2015 Article 794Hyung ArdiNo ratings yet
- Admin,+10 +raihanah,+et+al +moxibustion+for+nausea+andDocument6 pagesAdmin,+10 +raihanah,+et+al +moxibustion+for+nausea+andFajar MustafaNo ratings yet
- At The Time of PublicationDocument2 pagesAt The Time of PublicationAmirul Ashraf Bin ShukeriNo ratings yet
- 5 Faqs TB Preventive TreatmentDocument4 pages5 Faqs TB Preventive TreatmentGrace RabinaNo ratings yet
- Primary Health Care 2 1232967837997879 3Document42 pagesPrimary Health Care 2 1232967837997879 3JL CalvinNo ratings yet
- TB treatment guidelines pregnancyDocument8 pagesTB treatment guidelines pregnancyErum KhanNo ratings yet
- 2016 Propofol. Pediatric Drug Information. UPTODATEDocument10 pages2016 Propofol. Pediatric Drug Information. UPTODATEJoseloNo ratings yet
- Invanz Epar Product Information enDocument32 pagesInvanz Epar Product Information enanaNo ratings yet
- TB Treatment in India - New Patients, Previously Treated, Daily TreatmentDocument8 pagesTB Treatment in India - New Patients, Previously Treated, Daily Treatmentnaga tanoojNo ratings yet
- Anaesthesia - 2020 - Mitchell - Guideline On Anaesthesia and Sedation in Breastfeeding Women 2020Document12 pagesAnaesthesia - 2020 - Mitchell - Guideline On Anaesthesia and Sedation in Breastfeeding Women 2020ANGELICANo ratings yet
- Technical Update on the Integrated Management of Childhood Illness (IMCI) ProtocolDocument5 pagesTechnical Update on the Integrated Management of Childhood Illness (IMCI) ProtocolJaypee Ravina100% (2)
- Sangita Shrestha Manisha Dhungana: Prepared byDocument37 pagesSangita Shrestha Manisha Dhungana: Prepared byBhawna JoshiNo ratings yet
- A Practical Guide to Insulin Pump Therapy for PregnancyFrom EverandA Practical Guide to Insulin Pump Therapy for PregnancyNo ratings yet
- BLL in BhutanDocument8 pagesBLL in BhutanTob JurNo ratings yet
- Nutrition and VitaminDocument70 pagesNutrition and VitaminTob JurNo ratings yet
- Complete newborn exam guideDocument123 pagesComplete newborn exam guideSarahNo ratings yet
- 2019 Advanced Pead Nursing - Learning ModuleDocument16 pages2019 Advanced Pead Nursing - Learning ModuleTob JurNo ratings yet
- Pe AbdominalexamdgfhgjhkDocument20 pagesPe AbdominalexamdgfhgjhkMuhammed BarznjiNo ratings yet
- Nutrition and VitaminDocument70 pagesNutrition and VitaminTob JurNo ratings yet
- EnzymeDocument27 pagesEnzymeTob JurNo ratings yet
- Proteins: DR Sonam Chhoden RDocument33 pagesProteins: DR Sonam Chhoden RTob JurNo ratings yet
- Proteins: DR Sonam Chhoden RDocument33 pagesProteins: DR Sonam Chhoden RTob JurNo ratings yet
- Ca Colon 6Document28 pagesCa Colon 6Tob JurNo ratings yet
- Nutrition and safety risks for patient with stoma and low potassiumDocument23 pagesNutrition and safety risks for patient with stoma and low potassiumCzarina Porciuncula79% (14)
- Concept Mapping: A GPS for Patient Care in Various Healthcare EnvironmentsDocument39 pagesConcept Mapping: A GPS for Patient Care in Various Healthcare EnvironmentsTob JurNo ratings yet
- Colon Ca 5 PDFDocument9 pagesColon Ca 5 PDFTob JurNo ratings yet
- Cultivating Mindfulness of Bodhichitta c5 PDFDocument12 pagesCultivating Mindfulness of Bodhichitta c5 PDFTob JurNo ratings yet
- Nursing Care for Ostomy and Nutrition ManagementDocument4 pagesNursing Care for Ostomy and Nutrition ManagementTob JurNo ratings yet
- Pe AbdominalexamdgfhgjhkDocument20 pagesPe AbdominalexamdgfhgjhkMuhammed BarznjiNo ratings yet
- Academic Essay StructuresDocument2 pagesAcademic Essay StructuressershxNo ratings yet
- Nursing Care Plan Colorectal CancerDocument2 pagesNursing Care Plan Colorectal Cancerderic88% (34)
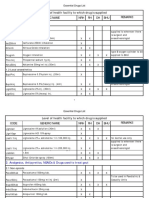
- Essential Drugs List by Facility LevelDocument42 pagesEssential Drugs List by Facility LevelTob JurNo ratings yet
- Assignment For Universal Value and Professional Ethics in NursingDocument5 pagesAssignment For Universal Value and Professional Ethics in NursingTob JurNo ratings yet
- Berry Dissertation PDFDocument187 pagesBerry Dissertation PDFTob JurNo ratings yet
- Finn 228Document12 pagesFinn 228Tob JurNo ratings yet
- Ca Colon 2Document19 pagesCa Colon 2Tob JurNo ratings yet
- 2019 Advanced Pead Nursing - Learning ModuleDocument16 pages2019 Advanced Pead Nursing - Learning ModuleTob JurNo ratings yet
- 2019 Advanced Pead Nursing - Learning ModuleDocument16 pages2019 Advanced Pead Nursing - Learning ModuleTob JurNo ratings yet
- Antenatal Summary VisitsDocument2 pagesAntenatal Summary VisitsTob JurNo ratings yet
- Antenatal Summary Visits PDFDocument2 pagesAntenatal Summary Visits PDFTob JurNo ratings yet
- A Review On Translation Strategies of Little Prince' by Ahmad Shamlou and Abolhasan NajafiDocument9 pagesA Review On Translation Strategies of Little Prince' by Ahmad Shamlou and Abolhasan Najafiinfo3814No ratings yet
- Administrative Law SyllabusDocument14 pagesAdministrative Law SyllabusKarl Lenin BenignoNo ratings yet
- TorricelliDocument35 pagesTorricelliAdinda Kayla Salsabila PutriNo ratings yet
- Module 6: 4M'S of Production and Business ModelDocument43 pagesModule 6: 4M'S of Production and Business ModelSou MeiNo ratings yet
- Digital Movement Guide CodesDocument18 pagesDigital Movement Guide Codescgeorgiou80No ratings yet
- Activity 1 DIASSDocument3 pagesActivity 1 DIASSLJ FamatiganNo ratings yet
- Operational Risk Roll-OutDocument17 pagesOperational Risk Roll-OutLee WerrellNo ratings yet
- Technical Contract for 0.5-4X1300 Slitting LineDocument12 pagesTechnical Contract for 0.5-4X1300 Slitting LineTjNo ratings yet
- Prac Research Module 2Document12 pagesPrac Research Module 2Dennis Jade Gascon NumeronNo ratings yet
- Wonder at The Edge of The WorldDocument3 pagesWonder at The Edge of The WorldLittle, Brown Books for Young Readers0% (1)
- The Awesome Life Force 1984Document8 pagesThe Awesome Life Force 1984Roman PetersonNo ratings yet
- Device Exp 2 Student ManualDocument4 pagesDevice Exp 2 Student Manualgg ezNo ratings yet
- IB Theatre: The Ilussion of InclusionDocument15 pagesIB Theatre: The Ilussion of InclusionLazar LukacNo ratings yet
- 2Document5 pages2Frances CiaNo ratings yet
- Consumer Behavior Paper PLDTDocument6 pagesConsumer Behavior Paper PLDTAngeline Santiago100% (2)
- ILOILO STATE COLLEGE OF FISHERIES-DUMANGAS CAMPUS ON-THE JOB TRAINING NARRATIVE REPORTDocument54 pagesILOILO STATE COLLEGE OF FISHERIES-DUMANGAS CAMPUS ON-THE JOB TRAINING NARRATIVE REPORTCherry Lyn Belgira60% (5)
- Topic 1 in 21st CneturyDocument8 pagesTopic 1 in 21st CneturyLuwisa RamosNo ratings yet
- Final Key 2519Document2 pagesFinal Key 2519DanielchrsNo ratings yet
- Skin Yale University Protein: Where Does Collagen Come From?Document2 pagesSkin Yale University Protein: Where Does Collagen Come From?Ellaine Pearl AlmillaNo ratings yet
- HERMAgreenGuide EN 01Document4 pagesHERMAgreenGuide EN 01PaulNo ratings yet
- AFRICAN SYSTEMS OF KINSHIP AND MARRIAGEDocument34 pagesAFRICAN SYSTEMS OF KINSHIP AND MARRIAGEjudassantos100% (2)
- Casey at The BatDocument2 pagesCasey at The BatGab SorianoNo ratings yet
- The Future of Indian Economy Past Reforms and Challenges AheadDocument281 pagesThe Future of Indian Economy Past Reforms and Challenges AheadANJALINo ratings yet
- Labov-DIFUSÃO - Resolving The Neogrammarian ControversyDocument43 pagesLabov-DIFUSÃO - Resolving The Neogrammarian ControversyGermana RodriguesNo ratings yet
- 1 - Nature and Dev - Intl LawDocument20 pages1 - Nature and Dev - Intl Lawaditya singhNo ratings yet
- PHEI Yield Curve: Daily Fair Price & Yield Indonesia Government Securities November 2, 2020Document3 pagesPHEI Yield Curve: Daily Fair Price & Yield Indonesia Government Securities November 2, 2020Nope Nope NopeNo ratings yet
- ACS Tech Manual Rev9 Vol1-TACTICS PDFDocument186 pagesACS Tech Manual Rev9 Vol1-TACTICS PDFMihaela PecaNo ratings yet
- Jaap Rousseau: Master ExtraodinaireDocument4 pagesJaap Rousseau: Master ExtraodinaireKeithBeavonNo ratings yet
- Megha Rakheja Project ReportDocument40 pagesMegha Rakheja Project ReportMehak SharmaNo ratings yet
- 1.1.1 Adverb Phrase (Advp)Document2 pages1.1.1 Adverb Phrase (Advp)mostarjelicaNo ratings yet