You might also like
- Clinical Approach To Lymphadenopathy: Annals of Nigerian Medicine January 2012Document8 pagesClinical Approach To Lymphadenopathy: Annals of Nigerian Medicine January 2012Aisyah DewiNo ratings yet
- Regimen MDR UpdateDocument35 pagesRegimen MDR UpdateAisyah DewiNo ratings yet
- Lower Extremity AmputationsDocument9 pagesLower Extremity AmputationsAisyah DewiNo ratings yet
- 155 (Phelps, Andrew)Document63 pages155 (Phelps, Andrew)Aisyah DewiNo ratings yet
- Gallstonepancreatitis:: A ReviewDocument24 pagesGallstonepancreatitis:: A ReviewAisyah DewiNo ratings yet
- EspenDocument235 pagesEspenAisyah DewiNo ratings yet
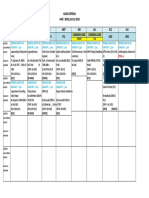
- Acara Operasi Hari: Senin, 13 Agustus 2018Document1 pageAcara Operasi Hari: Senin, 13 Agustus 2018Aisyah DewiNo ratings yet
- Droste 2007Document4 pagesDroste 2007Aisyah DewiNo ratings yet
- Acara Operasi Hari: Senin, 16 Juli 2018Document1 pageAcara Operasi Hari: Senin, 16 Juli 2018Aisyah DewiNo ratings yet
- DocumentDocument13 pagesDocumentAisyah DewiNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Fat CatsDocument7 pagesThe Fat CatsMarilo Jimenez AlgabaNo ratings yet
- MalachiteDocument2 pagesMalachiteAkhil KumarNo ratings yet
- N Methylpyrrolidone: Chemical Synonym General InformationDocument5 pagesN Methylpyrrolidone: Chemical Synonym General InformationMohamed AdelNo ratings yet
- Sdo Tle Grade 8 Dressmaking 2nd Q Week 1 8 1Document64 pagesSdo Tle Grade 8 Dressmaking 2nd Q Week 1 8 1Maggie De jesusNo ratings yet
- Acc05 SCG116Document42 pagesAcc05 SCG116Hilal HazaaNo ratings yet
- HPLC Columns by SciencixDocument49 pagesHPLC Columns by SciencixBrett HarrisNo ratings yet
- Acoustic Phonetics PDFDocument82 pagesAcoustic Phonetics PDFAnonymous mOSDA2100% (2)
- Anatomia Dezvoltarii PancreasuluiDocument49 pagesAnatomia Dezvoltarii Pancreasuluitarra abuNo ratings yet
- Regulatory Framework For Water Dams in QuebecDocument2 pagesRegulatory Framework For Water Dams in QuebecRaveeNo ratings yet
- One - Touch Fittings: Series: WP2Document12 pagesOne - Touch Fittings: Series: WP2PrashantNo ratings yet
- Curriculum Jaime Alvarado (Jaime Alvarado)Document3 pagesCurriculum Jaime Alvarado (Jaime Alvarado)yuly aldanaNo ratings yet
- Block-1 BLIS-03 Unit-2 PDFDocument15 pagesBlock-1 BLIS-03 Unit-2 PDFravinderreddynNo ratings yet
- Manual For Noncommissioned Officers and Privates of Infantry of The Army of The United StatesDocument250 pagesManual For Noncommissioned Officers and Privates of Infantry of The Army of The United StatesGutenberg.org100% (1)
- 7 Stages of NafsDocument7 pages7 Stages of NafsLilyNo ratings yet
- O221771s - Mil Pipe Pro 450 RFC PDFDocument84 pagesO221771s - Mil Pipe Pro 450 RFC PDFJavier Isaac Berrocal Torres100% (1)
- Nastran Preference Guide Volume 1 Structural AnalysisDocument724 pagesNastran Preference Guide Volume 1 Structural AnalysisGuido RossiNo ratings yet
- Origami Undergrad ThesisDocument63 pagesOrigami Undergrad ThesisEduardo MullerNo ratings yet
- Chem 3052 CHAPTER 7 (Nuclear Magnetic Resonance Spectroscopy (NMR) )Document6 pagesChem 3052 CHAPTER 7 (Nuclear Magnetic Resonance Spectroscopy (NMR) )ashenafiNo ratings yet
- 1 Soundcraft Notepad User GuideDocument40 pages1 Soundcraft Notepad User GuideNives KurjakNo ratings yet
- Schrodinger Wave EquationsDocument6 pagesSchrodinger Wave EquationsksksvtNo ratings yet
- An Overview of The IEEE Color BooksDocument6 pagesAn Overview of The IEEE Color BooksOhm666No ratings yet
- 7MBR75VB120-50: IGBT MODULE (V Series) 1200V / 75A / PIMDocument8 pages7MBR75VB120-50: IGBT MODULE (V Series) 1200V / 75A / PIMDanielle ButlerNo ratings yet
- The Redesigning of Junction: Tatya Tope Square BhopalDocument15 pagesThe Redesigning of Junction: Tatya Tope Square BhopalAr Raj YamgarNo ratings yet
- Cracked Tooth Syndrome. Part 1 Aetiology and DiagnosisDocument17 pagesCracked Tooth Syndrome. Part 1 Aetiology and Diagnosisfloressam2000No ratings yet
- Detailed Lesson Plan in Science IiiDocument3 pagesDetailed Lesson Plan in Science Iiicharito riveraNo ratings yet
- Course Specification Course Title: Basic Architectural DraftingDocument1 pageCourse Specification Course Title: Basic Architectural DraftingDinah Fe Tabaranza-OlitanNo ratings yet
- 12.1 ANSYS CompositePrepPostDocument2 pages12.1 ANSYS CompositePrepPostLakmal ArandaraNo ratings yet
- Fluid Mechanics & Machines - by LearnEngineering - inDocument307 pagesFluid Mechanics & Machines - by LearnEngineering - inVishva PatelNo ratings yet
- CH Six Global Transportation Planning and ExecutionDocument41 pagesCH Six Global Transportation Planning and ExecutionDsh ShNo ratings yet
- Methanol Technologies of Tkis: A Brief OverviewDocument12 pagesMethanol Technologies of Tkis: A Brief OverviewMuhammad NaeemNo ratings yet