You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Refrensi Trauma KemihDocument1 pageRefrensi Trauma KemihMoch. Ivan KurniawanNo ratings yet
- Refrensi Trauma KemihDocument1 pageRefrensi Trauma KemihMoch. Ivan KurniawanNo ratings yet
- Unit 3 DiathermyDocument63 pagesUnit 3 DiathermyAan Ika SugathotNo ratings yet
- Seven JumpDocument22 pagesSeven JumpMoch. Ivan KurniawanNo ratings yet
- Jurnal Dr. BaoDocument13 pagesJurnal Dr. BaoMoch. Ivan KurniawanNo ratings yet
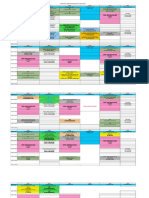
- Jadwal Blok THT Mata 2017 (1) Edit 1Document4 pagesJadwal Blok THT Mata 2017 (1) Edit 1Moch. Ivan KurniawanNo ratings yet
- BIO Chem Physio D I S E A S EDocument4 pagesBIO Chem Physio D I S E A S EMoch. Ivan KurniawanNo ratings yet
- Jadwal Blok Tropmed Sem 7 FK UHT 2017-2018Document5 pagesJadwal Blok Tropmed Sem 7 FK UHT 2017-2018Moch. Ivan KurniawanNo ratings yet
- Blepharitis 4Document2 pagesBlepharitis 4Moch. Ivan KurniawanNo ratings yet
- Journal Reading KulitDocument6 pagesJournal Reading KulitsintamirosmalindaNo ratings yet
- Ocular Toxoplasmosis - An Update and Review of The LiteratureDocument6 pagesOcular Toxoplasmosis - An Update and Review of The LiteratureMoch. Ivan KurniawanNo ratings yet
- Conjugata VeraDocument21 pagesConjugata VeraMoch. Ivan KurniawanNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
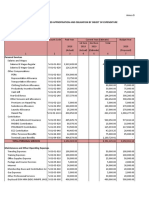
- Programmed Appropriation and Obligation by Object of ExpenditureDocument7 pagesProgrammed Appropriation and Obligation by Object of ExpenditureKristin Villaseñor-MercadoNo ratings yet
- Contaminarea Cu MelaninaDocument8 pagesContaminarea Cu Melaninadiana fenichiuNo ratings yet
- Sheetrock All Purpose Joint Compound Msds en 61320001Document8 pagesSheetrock All Purpose Joint Compound Msds en 61320001Andrew EnriquezNo ratings yet
- PLCO Cancer Screening Trial Medication QuestionnaireDocument3 pagesPLCO Cancer Screening Trial Medication QuestionnaireGeede AlfonsoNo ratings yet
- Department of A HospitalDocument24 pagesDepartment of A HospitalAnonymous YcdK9FWtH100% (2)
- 07 The Molecular Biology of CancerDocument39 pages07 The Molecular Biology of CancerJustin GonzalesNo ratings yet
- Can gray hair be donated for cancer wigsDocument1 pageCan gray hair be donated for cancer wigsDawa TsheringNo ratings yet
- Coronary Heart Disease: Angina Pectoris: Assistant Professor Department of Internal Medicine #1Document48 pagesCoronary Heart Disease: Angina Pectoris: Assistant Professor Department of Internal Medicine #1nadhirahfauzi100% (1)
- Compounded Sterile Products Stability Compendium-AntineoplasticsDocument0 pagesCompounded Sterile Products Stability Compendium-AntineoplasticsRahmalia 'lia Cudby' PrihanantoNo ratings yet
- Vasculitic Disorders: Dra. MezaDocument47 pagesVasculitic Disorders: Dra. MezaAna Beatriz Meza OntiverosNo ratings yet
- Virtual EAV: The Electro-Dermal Screening TestDocument21 pagesVirtual EAV: The Electro-Dermal Screening Testmich100% (1)
- Portal HypertensionDocument60 pagesPortal HypertensionParul VarshneyNo ratings yet
- Enlarged Peripheral Nerves On LeprosyDocument6 pagesEnlarged Peripheral Nerves On LeprosyGarrett SimpsonNo ratings yet
- Blood tests help diagnose diseasesDocument10 pagesBlood tests help diagnose diseasesMay Mawzi WahabNo ratings yet
- Chapman's Reflexes and Modern Clinical ApplicationsDocument94 pagesChapman's Reflexes and Modern Clinical ApplicationsYuldash100% (1)
- Comparing Chronological, Cause-Effect, and Compare-Contrast OrdersDocument3 pagesComparing Chronological, Cause-Effect, and Compare-Contrast OrdersIpha BadjaNo ratings yet
- Effects of Pollution Sample EssayDocument2 pagesEffects of Pollution Sample EssaybeNo ratings yet
- Breast milk jaundice causes and treatmentDocument3 pagesBreast milk jaundice causes and treatmentLembah BarokahNo ratings yet
- VaricoceleDocument3 pagesVaricoceleMandy ChengNo ratings yet
- Referat SLEDocument24 pagesReferat SLENihayatulHusniaNo ratings yet
- Hirschsprung's Disease - Congenital Mega Colon ExplainedDocument22 pagesHirschsprung's Disease - Congenital Mega Colon ExplainedHerry PriyantoNo ratings yet
- Athletes at High AltitudeDocument7 pagesAthletes at High AltitudeRodulfo AlvaradoNo ratings yet
- Posted: Mon Jun 21, 2010 4:02 PM Post Subject: DENTAL MCQS: Previous Year PaperDocument16 pagesPosted: Mon Jun 21, 2010 4:02 PM Post Subject: DENTAL MCQS: Previous Year PaperMadhul Singhal100% (1)
- Risk Assessment CalculatorDocument220 pagesRisk Assessment CalculatorTommaso BoedduNo ratings yet
- Life Expectancy FactorsDocument3 pagesLife Expectancy FactorsRizza GonzagaNo ratings yet
- JournalDocument17 pagesJournaljust for download matterNo ratings yet
- Kjjhhgfdsasdf HJKLKJHGFDSSDFG HJKLDocument4 pagesKjjhhgfdsasdf HJKLKJHGFDSSDFG HJKLbubble_inNo ratings yet
- Inflammatory Bowel DiseaseDocument25 pagesInflammatory Bowel DiseaseAndrew WdsmithNo ratings yet
- HESI Exit and NCLEX Exam GemsDocument21 pagesHESI Exit and NCLEX Exam GemsAntonella Vitale95% (80)
- Gamna Gandy BodiesDocument5 pagesGamna Gandy BodiesTaufik ShidkiNo ratings yet