You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Mastering Your Fears and Phobias - Therapist GuideDocument174 pagesMastering Your Fears and Phobias - Therapist Guidejesus100% (3)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Psychology WebDocument27 pagesPsychology WebしまののえだにNo ratings yet
- MHNPC (April 2014) Term 2 Individual Structured Therapy Activity PlanDocument6 pagesMHNPC (April 2014) Term 2 Individual Structured Therapy Activity PlanAiweiCheong100% (1)
- Activity Guide and Evaluation Rubric - Unit 1 - Task 2 - Picking Up Word ForumDocument18 pagesActivity Guide and Evaluation Rubric - Unit 1 - Task 2 - Picking Up Word ForumYoly HolguinNo ratings yet
- Henry Nnorom. Electronic Health Records (2021SU) Summer 2021Document4 pagesHenry Nnorom. Electronic Health Records (2021SU) Summer 2021henry nnoromNo ratings yet
- Annual Report - Dr. ReddysDocument62 pagesAnnual Report - Dr. ReddysSan DeepNo ratings yet
- Books ListsDocument7 pagesBooks ListsMiguel Cadagan100% (1)
- MHI2017 Assignment 4Document19 pagesMHI2017 Assignment 4Dr. Aby Mathews MaluvelilNo ratings yet
- Danish Study Shows No Benefit To Overall Mortality From mRNA VaccinesDocument13 pagesDanish Study Shows No Benefit To Overall Mortality From mRNA VaccinesJun KedNo ratings yet
- Application LetterDocument3 pagesApplication Letterangraini wulandari50% (2)
- Capstone PaperDocument16 pagesCapstone Paperapi-403963757No ratings yet
- Country Profile WorksheetDocument5 pagesCountry Profile WorksheetSun A LeeNo ratings yet
- OrganDocument391 pagesOrganmonimoy100% (1)
- AIA Mediguard Clinics With TCM - General (040111)Document11 pagesAIA Mediguard Clinics With TCM - General (040111)kunalcsNo ratings yet
- Grade 10 Long Quiz 4TH GradingDocument2 pagesGrade 10 Long Quiz 4TH Gradingjolina talledoNo ratings yet
- Executive Summary (ABC)Document1 pageExecutive Summary (ABC)Zi Jin HewNo ratings yet
- Daniel A. Schaffer 1351 Ne Miami GardensDocument5 pagesDaniel A. Schaffer 1351 Ne Miami GardensmdanmayNo ratings yet
- Theories NursingDocument1 pageTheories NursingFilipinas Sta MariaNo ratings yet
- Veteran Help-Seeking Behaviour For Mental HealthDocument6 pagesVeteran Help-Seeking Behaviour For Mental HealthDaniel KoffmanNo ratings yet
- A Seminar About History TakingDocument13 pagesA Seminar About History Takingdr_jamal1983No ratings yet
- Authorised Representative License: Executive Department of Registration and LicensingDocument1 pageAuthorised Representative License: Executive Department of Registration and LicensingFERAS ALSAMAKNo ratings yet
- Bicalutamide Monograph 1october2011Document5 pagesBicalutamide Monograph 1october2011shorfuddinfcc7816No ratings yet
- RRL and RRSDocument6 pagesRRL and RRSJAY LORRAINE PALACATNo ratings yet
- Importance of Soft Skill in WorkplaceDocument8 pagesImportance of Soft Skill in WorkplaceliliyayanonoNo ratings yet
- This Study Resource WasDocument2 pagesThis Study Resource WasAbhishek SachdevaNo ratings yet
- NCM110 NI CompiledNotesDocument6 pagesNCM110 NI CompiledNotesSherinne Jane CariazoNo ratings yet
- Temporomandibular DisordersDocument45 pagesTemporomandibular DisordersMohsin HabibNo ratings yet
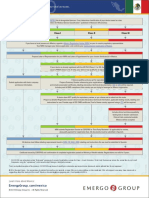
- Low Risk Class I Class II Class IIIDocument2 pagesLow Risk Class I Class II Class IIImd edaNo ratings yet
- A Manual For Implementation: Workload Indicators of Staffing Need (WISN)Document131 pagesA Manual For Implementation: Workload Indicators of Staffing Need (WISN)Ikhsan AkbarNo ratings yet
- Food Safety PosterDocument1 pageFood Safety PosterMP CariappaNo ratings yet