You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- 134 2013 Article 2998Document3 pages134 2013 Article 2998aditya brahmantio sujakaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Premed ConsiderationDocument9 pagesPremed Considerationaditya brahmantio sujakaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Penghitungan Total SKS, Sp2 Departemen Anestesi Semester Genap BenarDocument15 pagesPenghitungan Total SKS, Sp2 Departemen Anestesi Semester Genap Benaraditya brahmantio sujakaNo ratings yet
- RSU Haji Surabaya RSU Haji Surabaya RSU Haji SurabayaDocument1 pageRSU Haji Surabaya RSU Haji Surabaya RSU Haji Surabayaaditya brahmantio sujakaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Judul Acara DLLDocument1 pageJudul Acara DLLaditya brahmantio sujakaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
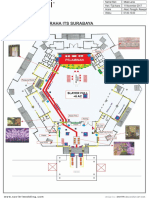
- Peta Graha ItsDocument1 pagePeta Graha Itsaditya brahmantio sujakaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- ITS Stage Edit LA 11 NeeeeeDocument1 pageITS Stage Edit LA 11 Neeeeeaditya brahmantio sujakaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Trauma OkuliDocument50 pagesTrauma Okuliaditya brahmantio sujakaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- PTC Course ManualDocument64 pagesPTC Course Manualaditya brahmantio sujakaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Undangan Seminar Internasional 2021-DikonversiDocument4 pagesUndangan Seminar Internasional 2021-DikonversiJandi PermadiNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Ministry of Health Begins Recruitment For Barbados Nursing JobsDocument2 pagesMinistry of Health Begins Recruitment For Barbados Nursing JobsKweku ZurekNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- GIT Conditions - StudentsDocument57 pagesGIT Conditions - StudentsShamal KoyeNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- 30.D18 788 Winny Yohana Indonesia-3-1Document4 pages30.D18 788 Winny Yohana Indonesia-3-1Yaumil FauziahNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Forcep Delivery..Document3 pagesForcep Delivery..Kristelle Joy Capili SicatNo ratings yet
- ResumeDocument1 pageResumeapi-353709440No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Abbott Alinity S FactSheetDocument1 pageAbbott Alinity S FactSheetInayat UllahNo ratings yet
- Ready To Use Tisseel - Quick Reference GuideDocument2 pagesReady To Use Tisseel - Quick Reference Guidebanguncitayam100% (1)
- 5 Minute Veterinary Consult Canine and FelineDocument1,016 pages5 Minute Veterinary Consult Canine and FelineMallory Bernstein100% (16)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- أساسيات التمريض نظرى (1) (1) 2222Document8 pagesأساسيات التمريض نظرى (1) (1) 2222Pŕìncëş Ğï ŘlNo ratings yet
- Pathophysiology of IBDDocument11 pagesPathophysiology of IBDOktarina Heni SunandarNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Nursing Care Plan Nursing Diagnosis Analysis Goal Intervention Rationale EvaluationDocument7 pagesNursing Care Plan Nursing Diagnosis Analysis Goal Intervention Rationale EvaluationHanz Abbigail Roco100% (1)
- Nursing at Harvard UNY 2Document4 pagesNursing at Harvard UNY 2Drajat FebrianNo ratings yet
- Korea Ghsa 2019Document283 pagesKorea Ghsa 2019BRAAAP SQRTNo ratings yet
- Kertas Penerangan: Program'S Code & NameDocument4 pagesKertas Penerangan: Program'S Code & NamearefifNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Bulletproof Cannabis PrescribingDocument30 pagesBulletproof Cannabis PrescribingstonerhinoNo ratings yet
- Basic Principles of NaturopathyDocument18 pagesBasic Principles of NaturopathyKanak Soni100% (2)
- 3 - Full Pulpotomy With Biodentine in Symptomatic Young Permanent Teeth With Carious Exposure PDFDocument6 pages3 - Full Pulpotomy With Biodentine in Symptomatic Young Permanent Teeth With Carious Exposure PDFAbdul Rahman AlmishhdanyNo ratings yet
- Nursing Bullets 5Document268 pagesNursing Bullets 5kate annNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- APhA Immunization Module 2Document12 pagesAPhA Immunization Module 2Gerald GamboaNo ratings yet
- Cadila Healthcare - WikipediaDocument14 pagesCadila Healthcare - WikipediaNUTHI SIVA SANTHAN100% (1)
- Spondyloarthropathies - Ankylosing Spondylitis, Psoriatic Arthritis, Reactive-Enteropathic Arthritis and HLA-B27 2020 PDFDocument125 pagesSpondyloarthropathies - Ankylosing Spondylitis, Psoriatic Arthritis, Reactive-Enteropathic Arthritis and HLA-B27 2020 PDFFazal Dalal100% (1)
- Nursing Exam Questions 2023 Part 1Document4 pagesNursing Exam Questions 2023 Part 1Lejo Sunny100% (1)
- PruBSN HEP+ BrochureDocument18 pagesPruBSN HEP+ BrochureMalik TaufiqNo ratings yet
- 2021-Myocarditis, Pericarditis and Cardiomyopathy After COVID-19 VaccinationDocument5 pages2021-Myocarditis, Pericarditis and Cardiomyopathy After COVID-19 Vaccinationseguridadyambiente641No ratings yet
- CollegePharmacy QuickGuideDocument16 pagesCollegePharmacy QuickGuideAnna WangNo ratings yet
- Adult CardDocument4 pagesAdult CardagelsantosNo ratings yet
- Hafid M. Jabir 18710093Document28 pagesHafid M. Jabir 18710093titin setya ningsihNo ratings yet
- Inc Tnai IcnDocument7 pagesInc Tnai IcnDeena MelvinNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Profile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyDocument6 pagesProfile of Tinea Corporis and Tinea Cruris in Dermatovenereology Clinic of Tertiery Hospital: A Retrospective StudyRose ParkNo ratings yet