You might also like
- Specific Heart Muscle DiseaseFrom EverandSpecific Heart Muscle DiseaseCecil SymonsNo ratings yet
- Clinical Case Ventricular Tachycardia Vet Team Brief 2016Document6 pagesClinical Case Ventricular Tachycardia Vet Team Brief 2016Katherina AdisaputroNo ratings yet
- Pathophysiology, Diagnosis and Treatment of TachycardiomyopathyDocument10 pagesPathophysiology, Diagnosis and Treatment of TachycardiomyopathyTemptationNo ratings yet
- Pathophysiology, Diagnosis and Treatment of TachycardiomyopathyDocument10 pagesPathophysiology, Diagnosis and Treatment of TachycardiomyopathydimasNo ratings yet
- Myocardial Infarction: Coronary Heart Disease (CHD) Coronary Artery Disease (CAD) Ischaemic Heart Disease (IHD)Document29 pagesMyocardial Infarction: Coronary Heart Disease (CHD) Coronary Artery Disease (CAD) Ischaemic Heart Disease (IHD)Mahum SohailNo ratings yet
- 26 CardiomyopathiesDocument44 pages26 CardiomyopathiesVictor PazNo ratings yet
- Linician Pdate: Catheter Ablation of Ventricular TachycardiaDocument6 pagesLinician Pdate: Catheter Ablation of Ventricular TachycardiaSonia Rahma ANo ratings yet
- Low Cardiac Output ChildrenDocument11 pagesLow Cardiac Output ChildrenXavier AbrilNo ratings yet
- Abstract and Introduction Journal Review AnastesiDocument38 pagesAbstract and Introduction Journal Review Anastesiaye ayeNo ratings yet
- Jurnal 1assasDocument4 pagesJurnal 1assasZul Qodri GintingNo ratings yet
- Prometric High-Yield NOTES PDFDocument135 pagesPrometric High-Yield NOTES PDFDr-Jahanzaib Gondal100% (3)
- Terapia Dirigida IccDocument11 pagesTerapia Dirigida Iccalejandro montesNo ratings yet
- DCM - Current TreatmentDocument9 pagesDCM - Current TreatmentSri NathNo ratings yet
- CardiomyopathiesDocument13 pagesCardiomyopathiesNinna Isabel VictorioNo ratings yet
- Cardiomyopathy & MyocarditisDocument329 pagesCardiomyopathy & MyocarditisAbnet WondimuNo ratings yet
- 2 Myocardial Infarction Nursing Care Management and Study GuideDocument13 pages2 Myocardial Infarction Nursing Care Management and Study GuideQuijano Gpokskie100% (2)
- IM - Cardiomyopathy and MyocarditisDocument9 pagesIM - Cardiomyopathy and MyocarditisElisha BernabeNo ratings yet
- Dilated CardiomyopathyDocument125 pagesDilated CardiomyopathyAbnet WondimuNo ratings yet
- Manajemen PVCDocument11 pagesManajemen PVCHarie CiptaNo ratings yet
- Cardiac Toxic ResponsesDocument10 pagesCardiac Toxic ResponsesDaismar ArenasNo ratings yet
- Cardiac TamponadeprintedDocument7 pagesCardiac TamponadeprintedGreen HanauNo ratings yet
- Falla CardiacaDocument6 pagesFalla CardiacaFelipeNo ratings yet
- Constrictive and Restrictive Cardiomyopathy PDFDocument19 pagesConstrictive and Restrictive Cardiomyopathy PDFdawnkuruvillaNo ratings yet
- Investigation and Management of Congestive Heart Failure: Clinical ReviewDocument6 pagesInvestigation and Management of Congestive Heart Failure: Clinical ReviewDwiky YuanasikaNo ratings yet
- AHA 2008 Shock CardiogenicDocument13 pagesAHA 2008 Shock CardiogenicbayuniNo ratings yet
- Module 17 Part 2 Ratio 19 22 EndoDocument102 pagesModule 17 Part 2 Ratio 19 22 EndoLA BriguelaNo ratings yet
- Penanganan Ima1Document81 pagesPenanganan Ima1Debbi AnggrainiNo ratings yet
- Cardio Onco ReviewDocument14 pagesCardio Onco ReviewFrancisco MonzonNo ratings yet
- Taponamiento CardiacoDocument9 pagesTaponamiento CardiacoLiz Aliaga KnutzenNo ratings yet
- A Mistake That Has Hurt No One: Sinus MistakusDocument4 pagesA Mistake That Has Hurt No One: Sinus MistakusasclepiuspdfsNo ratings yet
- Cardiomyopathies 6th Year Seminar GRP BBDocument42 pagesCardiomyopathies 6th Year Seminar GRP BBmohamedeen hamza100% (1)
- Cardiac-arrhythmias-in-the-critically-ill-adult--aDocument13 pagesCardiac-arrhythmias-in-the-critically-ill-adult--aAlia SandoQaNo ratings yet
- Pharmacokinetics and Pharmacodynamics PDFDocument166 pagesPharmacokinetics and Pharmacodynamics PDFCarolina PosadaNo ratings yet
- Antiarrhythmic-drugs_2024_mpaicDocument5 pagesAntiarrhythmic-drugs_2024_mpaicAlia SandoQaNo ratings yet
- CLC 42 484Document10 pagesCLC 42 484Heath HensleyNo ratings yet
- CLC 42 484Document10 pagesCLC 42 484Stijn VermoteNo ratings yet
- How To Detect and To Treat EarlierDocument59 pagesHow To Detect and To Treat EarlierFaisal ShaldyNo ratings yet
- The Feline Cardiomyopathies: 1. General ConceptsDocument19 pagesThe Feline Cardiomyopathies: 1. General ConceptsAna AldazNo ratings yet
- Fibrilación AuricularDocument9 pagesFibrilación AuricularMartin De Santiago ValenzuelaNo ratings yet
- Anesthesia For Dogs With Myxomatous Mitral Valve DiseaseDocument7 pagesAnesthesia For Dogs With Myxomatous Mitral Valve DiseaseMiguel MuunguiiaNo ratings yet
- Cardiomyopathies Valvular Heart Diseases MyocarditisDocument28 pagesCardiomyopathies Valvular Heart Diseases MyocarditisensiNo ratings yet
- Mitchell 2005Document8 pagesMitchell 2005DianNo ratings yet
- J Jacc 2019 11 028Document4 pagesJ Jacc 2019 11 028oky legyanNo ratings yet
- Uia 14 Anaesthesia For Patients With Cardiac Disease Undergoing Non Cardiac SurgeryDocument6 pagesUia 14 Anaesthesia For Patients With Cardiac Disease Undergoing Non Cardiac Surgerybhaskaracharya dontabhaktuniNo ratings yet
- Iadt03i5p345 PDFDocument15 pagesIadt03i5p345 PDFSudhit SethiNo ratings yet
- Diagnosis of Circulatory FailureDocument21 pagesDiagnosis of Circulatory FailureQuang Anh LeNo ratings yet
- DR Dhiman BanikCariogenic Shock Final 2022 DDDocument59 pagesDR Dhiman BanikCariogenic Shock Final 2022 DDCloudySkyNo ratings yet
- CirculatoryDocument13 pagesCirculatorysuelly-majorNo ratings yet
- Acute Coronary SyndromeDocument18 pagesAcute Coronary SyndromeKartika RahmawatiNo ratings yet
- Contemporary Reviews in Cardiovascular Medicine: Cardiogenic ShockDocument32 pagesContemporary Reviews in Cardiovascular Medicine: Cardiogenic ShockSindhuNugrohoMuktiNo ratings yet
- Perioperative Implications of Pericardial Effusions and Cardiac TamponadeDocument9 pagesPerioperative Implications of Pericardial Effusions and Cardiac TamponadeMarielou CoutinhoNo ratings yet
- Managing Atrial FibrillationDocument4 pagesManaging Atrial FibrillationHesbon MomanyiNo ratings yet
- 09.1 STEMI in Special Condition Young Age Pregnancy Renal Failure Rukma Juslim MD FIHADocument32 pages09.1 STEMI in Special Condition Young Age Pregnancy Renal Failure Rukma Juslim MD FIHARirin ArtantiNo ratings yet
- Med Surg Assignment 2Document69 pagesMed Surg Assignment 2sham gowliNo ratings yet
- 1 s2.0 S1936878X23000311 Main PDFDocument18 pages1 s2.0 S1936878X23000311 Main PDFCarmen Cuadros BeigesNo ratings yet
- Managementul Socului CardiogenDocument15 pagesManagementul Socului CardiogenDiana GosavNo ratings yet
- Case Study 01 Myocardial InfarctionDocument11 pagesCase Study 01 Myocardial InfarctionAldrin BardeNo ratings yet
- Shock CardiogenicoDocument15 pagesShock CardiogenicoGianny VGNo ratings yet
- RIHD AnatomyDocument8 pagesRIHD AnatomyAstrid Karina PutriNo ratings yet
- Cardiomyopathy and Anaesthesia PDFDocument6 pagesCardiomyopathy and Anaesthesia PDFZaky HasanNo ratings yet
- Sedation EngDocument17 pagesSedation EngZaky HasanNo ratings yet
- Cardiomyopathy and Anaesthesia PDFDocument6 pagesCardiomyopathy and Anaesthesia PDFZaky HasanNo ratings yet
- Anestesi Pada ChildDocument17 pagesAnestesi Pada ChildZaky HasanNo ratings yet
- Cardiovascular Agents: Florianne E. Adlawan, R.NDocument31 pagesCardiovascular Agents: Florianne E. Adlawan, R.NadlawanflorianneNo ratings yet
- Prof. M. Rushdi: PolycythemiaDocument6 pagesProf. M. Rushdi: PolycythemiaaymenNo ratings yet
- ECT Manual-NIMHANS Ed.2 Compressed-2Document70 pagesECT Manual-NIMHANS Ed.2 Compressed-2Utkarsh Modi50% (6)
- Suntext Complete Journal 2021Document35 pagesSuntext Complete Journal 2021Maruf HasanNo ratings yet
- Common Resuscitative DrugsDocument3 pagesCommon Resuscitative DrugsChris Jardine LiNo ratings yet
- Atrial Septal DefectDocument5 pagesAtrial Septal DefectalmorsNo ratings yet
- Traumatic Head InjuriesDocument50 pagesTraumatic Head InjuriesVasudha BuddyNo ratings yet
- Dressler's Syndrome:: A Rare ComplicationDocument3 pagesDressler's Syndrome:: A Rare ComplicationFitri Sri WulandariNo ratings yet
- Investigations in Oral MedicineDocument18 pagesInvestigations in Oral Medicinedr_jamal1983100% (2)
- Management of Hyperkalaemia and HypokalaemiaDocument21 pagesManagement of Hyperkalaemia and Hypokalaemiaferoza97No ratings yet
- Funda PostDocument10 pagesFunda PostChaina MacaspacNo ratings yet
- Test Bank For Quick and Easy Medical Terminology 8th Edition by LeonardDocument15 pagesTest Bank For Quick and Easy Medical Terminology 8th Edition by Leonardamyrileyixgnaoqjmt100% (20)
- Cardiology PDFDocument8 pagesCardiology PDFTran Chi TienNo ratings yet
- Health Assessment - Cardiovascular and Peripheral Vascular SystemsDocument5 pagesHealth Assessment - Cardiovascular and Peripheral Vascular SystemsPenelope E. Davidson100% (1)
- Nephro Gudie For HODocument22 pagesNephro Gudie For HOSarmad AsifNo ratings yet
- Drug StudyDocument49 pagesDrug StudyLexa Moreene Cu�adoNo ratings yet
- Nursing Care of Patients With Digestive & Gastrointestinal DisordersDocument29 pagesNursing Care of Patients With Digestive & Gastrointestinal DisordersjoreyneeNo ratings yet
- Biology Worksheet Sheep Heart DissectionDocument3 pagesBiology Worksheet Sheep Heart DissectionFluphie Bunny0% (1)
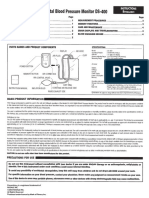
- Digital Blood Pressure Monitor DS-400: Parts Names and Product ComponentsDocument4 pagesDigital Blood Pressure Monitor DS-400: Parts Names and Product ComponentsJorNo ratings yet
- Review Assessment Quiz 1 Ischemic StrokeDocument4 pagesReview Assessment Quiz 1 Ischemic Strokelcastro8No ratings yet
- CDH and Pulmonary HypertensionDocument6 pagesCDH and Pulmonary HypertensionStollery SandboxNo ratings yet
- Physical Examination GI Track (INTERNATIONAL)Document59 pagesPhysical Examination GI Track (INTERNATIONAL)AnnisNo ratings yet
- Treatment For ICU WardDocument40 pagesTreatment For ICU Wardknowledge chanall chanallNo ratings yet
- Pathology, Lecture 2, Cell Injury (Slides)Document139 pagesPathology, Lecture 2, Cell Injury (Slides)Ali Al-Qudsi100% (8)
- Anatomy Physiology and Disease An Interactive Journey For Health Professions 2nd Edition Colbert Test BankDocument32 pagesAnatomy Physiology and Disease An Interactive Journey For Health Professions 2nd Edition Colbert Test BankAliciaMcintoshaeiop100% (13)
- Peripheral Vascular InterventionsDocument1,225 pagesPeripheral Vascular InterventionsAvinash6614No ratings yet
- Chronic Kidney Disease: A Case Presentation OnDocument16 pagesChronic Kidney Disease: A Case Presentation OnSafoora RafeeqNo ratings yet
- Epithelial and connective tissue types in the human bodyDocument4 pagesEpithelial and connective tissue types in the human bodyrenee belle isturisNo ratings yet
- Tocolytic Agents and Anticonvulsants for Preterm LabourDocument95 pagesTocolytic Agents and Anticonvulsants for Preterm LabourPriya jNo ratings yet
- Human Physiology 14Th Edition Fox Solutions Manual Full Chapter PDFDocument37 pagesHuman Physiology 14Th Edition Fox Solutions Manual Full Chapter PDFletitiaestheru3hnxz100% (8)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (31)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Secure Love: Create a Relationship That Lasts a LifetimeFrom EverandSecure Love: Create a Relationship That Lasts a LifetimeRating: 5 out of 5 stars5/5 (17)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)