You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Survival Analysis, Part 3: Cox Regression: Statistics and Research DesignDocument2 pagesSurvival Analysis, Part 3: Cox Regression: Statistics and Research DesignGloria KartikaNo ratings yet
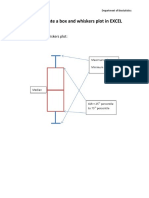
- How To Create A Box and Whiskers Plot in EXCELDocument9 pagesHow To Create A Box and Whiskers Plot in EXCELGloria KartikaNo ratings yet
- MC GowanDocument13 pagesMC GowanGloria KartikaNo ratings yet
- 24 Newsletter Hypertension and ArrhythmiaDocument2 pages24 Newsletter Hypertension and ArrhythmiaGloria KartikaNo ratings yet
- Insertion of An Intra-Aortic Balloon Catheter: PurposeDocument4 pagesInsertion of An Intra-Aortic Balloon Catheter: PurposeGloria KartikaNo ratings yet
- CLN 66 01 107 PDFDocument5 pagesCLN 66 01 107 PDFGloria KartikaNo ratings yet
- Staining and Tooth DiscolorationDocument14 pagesStaining and Tooth DiscolorationGloria KartikaNo ratings yet
- Hypertension: H.) or May Be Associated With Other Diseases - Dorland'sDocument1 pageHypertension: H.) or May Be Associated With Other Diseases - Dorland'sGloria KartikaNo ratings yet
- Infeksi Marginalis NadaDocument48 pagesInfeksi Marginalis NadaGloria KartikaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Eur J Echocardiogr 2010 Walker E37Document4 pagesEur J Echocardiogr 2010 Walker E37Muhammad Haryadi AdeNo ratings yet
- Cardiac Computed TomographyDocument29 pagesCardiac Computed TomographyAnu MavelyNo ratings yet
- Sliwa Et Al-2010-European Journal of Heart FailureDocument12 pagesSliwa Et Al-2010-European Journal of Heart FailurealfredoibcNo ratings yet
- Prorpt - S012018050017 - Echo 1 ProjectDocument3 pagesProrpt - S012018050017 - Echo 1 ProjectNur NabilaNo ratings yet
- Echocardiographic Anatomy in The FetusDocument14 pagesEchocardiographic Anatomy in The FetusAnonymous hOHi6TZTnNo ratings yet
- BSC CardtechDocument25 pagesBSC CardtechShahidriswanNo ratings yet
- Clozapina e MiocarditeDocument14 pagesClozapina e MiocarditeRafael Gaede CarrilloNo ratings yet
- Guidelines For Chamber QuantificationDocument1 pageGuidelines For Chamber QuantificationZoltán Tirczka100% (1)
- Basics of Functional Echocardiography in Children and NeonatesDocument13 pagesBasics of Functional Echocardiography in Children and Neonatestigtigrai49No ratings yet
- Di V V: Cardiomath Equations InfoDocument35 pagesDi V V: Cardiomath Equations InfoMd. ashfaque Ahemmed khanNo ratings yet
- Plain Time Table Update 11 September 2019Document59 pagesPlain Time Table Update 11 September 2019Lisaagustina GuiNo ratings yet
- Tarrass FDocument2 pagesTarrass FDr. Jatin GargNo ratings yet
- Advance ProgramDocument100 pagesAdvance ProgrambibNo ratings yet
- 2017 ASC Certification Sample Letter Fellowship PathwayDocument1 page2017 ASC Certification Sample Letter Fellowship PathwayfhkhattakNo ratings yet
- Cardio FellowDocument19 pagesCardio FellowJa GhNo ratings yet
- TOP 1000 CPT® CODES For ADULT NURSE PRACTITIONERSDocument4 pagesTOP 1000 CPT® CODES For ADULT NURSE PRACTITIONERSbritofernandezaNo ratings yet
- Infective Endocarditis (IE)Document76 pagesInfective Endocarditis (IE)Mahesh RathnayakeNo ratings yet
- CircleCVI-The 10-Min CMR Scan Business Opportunity AssessmentDocument58 pagesCircleCVI-The 10-Min CMR Scan Business Opportunity AssessmentQiao WeiNo ratings yet
- Cardio SNAP-BNP NT-proBNP IdexxDocument4 pagesCardio SNAP-BNP NT-proBNP IdexxXenia FernandezNo ratings yet
- Announcement List Displayed Poster 32nd ASMIHADocument36 pagesAnnouncement List Displayed Poster 32nd ASMIHADewi AmeliaNo ratings yet
- Sonovue H C 303 II 0025 Epar Assessment Report Variation - enDocument33 pagesSonovue H C 303 II 0025 Epar Assessment Report Variation - enWendy TaborNo ratings yet
- 38 Endocardial Cushion DefectsDocument12 pages38 Endocardial Cushion DefectsVictor PazNo ratings yet
- Echocardiography Review Guide Companion To The Textbook of Clinical Echocardiography 5E (2015) (PDF) (UnitedVRG) PDFDocument435 pagesEchocardiography Review Guide Companion To The Textbook of Clinical Echocardiography 5E (2015) (PDF) (UnitedVRG) PDFsavannah78100% (2)
- The Role of Echocardiographic Study in Patients With Chronic Kidney DiseaseDocument9 pagesThe Role of Echocardiographic Study in Patients With Chronic Kidney DiseaseshodhgangaNo ratings yet
- Vertebral Scale System To Measure Heart Size in Dogs in Thoracic RadiographsDocument4 pagesVertebral Scale System To Measure Heart Size in Dogs in Thoracic Radiographsludiegues752No ratings yet
- Final Announcement Book 26th ASMIHA 2017-1Document47 pagesFinal Announcement Book 26th ASMIHA 2017-1d.ramadhanNo ratings yet
- Acute and Chronic Heart FailureDocument61 pagesAcute and Chronic Heart FailureigohNo ratings yet
- Vijayalakshmi 2008Document7 pagesVijayalakshmi 2008Rakesh DashNo ratings yet
- Pulmonary Atresia With An Intact Ventricular Septum: Preoperative Physiology, Imaging, and ManagementDocument11 pagesPulmonary Atresia With An Intact Ventricular Septum: Preoperative Physiology, Imaging, and ManagementAkilaNo ratings yet
- 2011-2012 Annual ReportDocument131 pages2011-2012 Annual ReportSlusom WebNo ratings yet