You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- BCOM Lecture 1-21-2023Document34 pagesBCOM Lecture 1-21-2023EricNo ratings yet
- Green and Gracious Builder Guide (SMC)Document36 pagesGreen and Gracious Builder Guide (SMC)Jack LeeNo ratings yet
- Abdu'l-Bahá Abbás (1844-1921)Document15 pagesAbdu'l-Bahá Abbás (1844-1921)BVILLARNo ratings yet
- Quality of Life in Patients Implanted With The BAHA Device Depending On The AetiologyDocument5 pagesQuality of Life in Patients Implanted With The BAHA Device Depending On The AetiologyCarlos SotgiuNo ratings yet
- Bun338 Iss2 Sep16 Mfi Quick GuideDocument4 pagesBun338 Iss2 Sep16 Mfi Quick GuideCarlos SotgiuNo ratings yet
- Hearing Rehabilitation With The Closed Skin Bone-Anchored Implant Sophono Alpha1 - Results of A Prospective Study in 15 Children With Ear AtresiaDocument6 pagesHearing Rehabilitation With The Closed Skin Bone-Anchored Implant Sophono Alpha1 - Results of A Prospective Study in 15 Children With Ear AtresiaCarlos SotgiuNo ratings yet
- M Sur121Document9 pagesM Sur121Carlos SotgiuNo ratings yet
- Bone Anchored Hearing Implant - Aid - BAHI - BAHA - SurgeryDocument18 pagesBone Anchored Hearing Implant - Aid - BAHI - BAHA - SurgeryCarlos SotgiuNo ratings yet
- Bahai PrayersDocument103 pagesBahai PrayersTom Erwin100% (6)
- Abdu'l-Bahá Abbás (1844-1921)Document15 pagesAbdu'l-Bahá Abbás (1844-1921)BVILLARNo ratings yet
- Bahai PrayersDocument103 pagesBahai PrayersTom Erwin100% (6)
- BUN226 ISS2 JAN14 Attract Surgery Guide US TPDocument28 pagesBUN226 ISS2 JAN14 Attract Surgery Guide US TPhoneysutton8No ratings yet
- Bahai Enciclop Paz ConflictosDocument3 pagesBahai Enciclop Paz ConflictosCarlos SotgiuNo ratings yet
- Response of The Human Skull To Mechanical VibrationsDocument9 pagesResponse of The Human Skull To Mechanical VibrationsCarlos SotgiuNo ratings yet
- Response of The Human Skull To Mechanical VibrationsDocument9 pagesResponse of The Human Skull To Mechanical VibrationsCarlos SotgiuNo ratings yet
- Sound Wave Propagation On The Human Skull Surface With Bone Conduction StimulationDocument13 pagesSound Wave Propagation On The Human Skull Surface With Bone Conduction StimulationCarlos SotgiuNo ratings yet
- The Bone-Anchored Hearing Device (Baha)Document5 pagesThe Bone-Anchored Hearing Device (Baha)Carlos Sotgiu100% (1)
- Surgical Outcome of Bone Anchored Hearing Aid (Baha) Implant SurgeryDocument4 pagesSurgical Outcome of Bone Anchored Hearing Aid (Baha) Implant SurgeryCarlos SotgiuNo ratings yet
- The Current Practice Trends in Pediatric Bone-AnchDocument10 pagesThe Current Practice Trends in Pediatric Bone-AnchCarlos SotgiuNo ratings yet
- Intermediate Outcomes of A Transcutaneous Bone Conduction Hearing Device in A Paediatric PopulationDocument5 pagesIntermediate Outcomes of A Transcutaneous Bone Conduction Hearing Device in A Paediatric PopulationCarlos SotgiuNo ratings yet
- Transmission of Bone-Conducted SoundDocument65 pagesTransmission of Bone-Conducted SoundCarlos SotgiuNo ratings yet
- Cochlear Baha Attract System: Summary of Clinical Results and BenefitsDocument5 pagesCochlear Baha Attract System: Summary of Clinical Results and BenefitsCarlos SotgiuNo ratings yet
- The Physics of SoundDocument44 pagesThe Physics of SoundSakaiiWongNo ratings yet
- 100-Article Text-313-1-10-20100216 PDFDocument12 pages100-Article Text-313-1-10-20100216 PDFCarlos SotgiuNo ratings yet
- Hearing Rehabilitation in Congenital Canal AtresiaDocument5 pagesHearing Rehabilitation in Congenital Canal AtresiaCarlos SotgiuNo ratings yet
- Cochlear Baha Attract System: Summary of Clinical Results and BenefitsDocument5 pagesCochlear Baha Attract System: Summary of Clinical Results and BenefitsCarlos SotgiuNo ratings yet
- The Bone-Anchored Hearing Device (Baha)Document5 pagesThe Bone-Anchored Hearing Device (Baha)Carlos Sotgiu100% (1)
- Speech AudiometryDocument5 pagesSpeech Audiometry354No ratings yet
- 32311Document42 pages32311Jam Knows RightNo ratings yet
- Capitalism Vs CommunismDocument1 pageCapitalism Vs CommunismCarlos SotgiuNo ratings yet
- Itts Final ReviewerDocument30 pagesItts Final ReviewerShaira GrafilNo ratings yet
- Fuji Noise Level Analyzer: For FUJI Digital Sound Detector FSB-8DDocument2 pagesFuji Noise Level Analyzer: For FUJI Digital Sound Detector FSB-8DMar WilkNo ratings yet
- 188 ArticleText 561 1 10 20191029Document7 pages188 ArticleText 561 1 10 20191029khaled alahmadNo ratings yet
- Ccauv02 18 PDFDocument4 pagesCcauv02 18 PDFAldrin HernandezNo ratings yet
- Environmental LegislationsDocument121 pagesEnvironmental LegislationsFrancia VillarealNo ratings yet
- OldSiteOperators and ServiceSkidder620E (6206201-6209000) Service (6206201 - 6206400) 41336AENGDocument598 pagesOldSiteOperators and ServiceSkidder620E (6206201-6209000) Service (6206201 - 6206400) 41336AENGmarceloNo ratings yet
- Engineering Guide to Air Distribution SystemsDocument0 pagesEngineering Guide to Air Distribution SystemsmohdnazirNo ratings yet
- Manual GA116 GA216 GA257 Sonus Operating ManualDocument154 pagesManual GA116 GA216 GA257 Sonus Operating ManualTarun BhatiaNo ratings yet
- Deluca Surface Electromyography Detection&RecordingDocument10 pagesDeluca Surface Electromyography Detection&RecordingJuan Rodriguez IIINo ratings yet
- Jurnal 1Document9 pagesJurnal 1fadhil ramadhanNo ratings yet
- NZTA Noise Barriers v1.0Document82 pagesNZTA Noise Barriers v1.0jonrua100% (1)
- American Journal of Public Health, Marzo 1938Document22 pagesAmerican Journal of Public Health, Marzo 1938Gely ReyesNo ratings yet
- HSM 461en1Document174 pagesHSM 461en1Mtunzi MzamoNo ratings yet
- MEC 115 Noise Vibration&ControlDocument150 pagesMEC 115 Noise Vibration&ControlMauriceNo ratings yet
- RA Excessive Noise .Vibration.Document11 pagesRA Excessive Noise .Vibration.Ndifor Dinho0% (1)
- Instruction Manual Makita Rp0900Document12 pagesInstruction Manual Makita Rp0900Jonathan Pascua CamachoNo ratings yet
- Initial Environmental Audit Report - ReviewedDocument29 pagesInitial Environmental Audit Report - Reviewedmaxwell odhiamboNo ratings yet
- Plant and Equipment Risk Assessment Fgoc - NewDocument12 pagesPlant and Equipment Risk Assessment Fgoc - Newmajid khanNo ratings yet
- AFO AS POL 09 0001 - 2 0 Pedestrian SafetyDocument27 pagesAFO AS POL 09 0001 - 2 0 Pedestrian SafetymugishabobNo ratings yet
- Atlas Copco Portable Air Compressors: Series 7Document8 pagesAtlas Copco Portable Air Compressors: Series 7Fabumarinho26No ratings yet
- Fatima FertilizerDocument21 pagesFatima Fertilizerubaid shahNo ratings yet
- IS 14489 Check ListDocument17 pagesIS 14489 Check Listsathish_iyengarNo ratings yet
- Cutmaster 102: Operating ManualDocument84 pagesCutmaster 102: Operating ManualPabloNo ratings yet
- Matecconf Icmee2015 02001Document5 pagesMatecconf Icmee2015 02001NoLifeNo ratings yet
- Behaviour of Sound in An Enclosed SpaceDocument14 pagesBehaviour of Sound in An Enclosed Spacesanchit gupta100% (1)
- MRS51 PDFDocument14 pagesMRS51 PDFTim LynnNo ratings yet
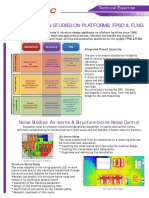
- Noise & Vibration Studies On Platforms, Fpso & FLNG: Noise Studies: Air-Borne & Structure-Borne Noise ControlDocument2 pagesNoise & Vibration Studies On Platforms, Fpso & FLNG: Noise Studies: Air-Borne & Structure-Borne Noise ControlNor Azlan AwangNo ratings yet
- Acoustics: BulletinDocument72 pagesAcoustics: BulletinYan MengNo ratings yet