You might also like
- Aspire To AchieveDocument11 pagesAspire To AchieveIndresh Singh SalujaNo ratings yet
- Job Description - DFMDocument3 pagesJob Description - DFMIndresh Singh SalujaNo ratings yet
- LSS YB Project TemplateDocument9 pagesLSS YB Project TemplateIndresh Singh SalujaNo ratings yet
- Questions - Analytics TestDocument1 pageQuestions - Analytics TestIndresh Singh SalujaNo ratings yet
- QFD Strategy Matrix - Servile RelocationsDocument7 pagesQFD Strategy Matrix - Servile RelocationsIndresh Singh SalujaNo ratings yet
- Retail Management: Private & Confidential For Use and Circulation Within Acorn Holdings LimitedDocument10 pagesRetail Management: Private & Confidential For Use and Circulation Within Acorn Holdings LimitedIndresh Singh SalujaNo ratings yet
- Analysis - Customer TenureDocument7 pagesAnalysis - Customer TenureIndresh Singh SalujaNo ratings yet
- LSS YB Project TemplateDocument9 pagesLSS YB Project TemplateIndresh Singh SalujaNo ratings yet
- Data and Analysis v4Document51 pagesData and Analysis v4Indresh Singh SalujaNo ratings yet
- Qwetu Analytical TestDocument16 pagesQwetu Analytical TestIndresh Singh SalujaNo ratings yet
- Practice Data For LEARNING STATISTICSDocument6 pagesPractice Data For LEARNING STATISTICSIndresh Singh SalujaNo ratings yet
- Sms ScriptsDocument6 pagesSms ScriptsIndresh Singh SalujaNo ratings yet
- Daily DashboardDocument141 pagesDaily DashboardIndresh Singh Saluja100% (1)
- Classification Scheme For Services Under GSTDocument37 pagesClassification Scheme For Services Under GSTArul PrakashNo ratings yet
- Lean Bread Making QuestionDocument4 pagesLean Bread Making QuestionIndresh Singh SalujaNo ratings yet
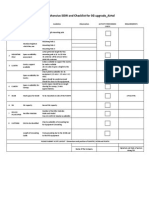
- Comprehensive SOW and Checklist For 3G Upgrade - AirtelDocument2 pagesComprehensive SOW and Checklist For 3G Upgrade - AirtelIndresh Singh SalujaNo ratings yet
- RTPL - Case StudyDocument13 pagesRTPL - Case StudyIndresh Singh SalujaNo ratings yet
- Excel GuideDocument208 pagesExcel GuideIndresh Singh SalujaNo ratings yet
- Lean 6 SigmaDocument17 pagesLean 6 SigmaIndresh Singh SalujaNo ratings yet
- Org Structure Small Fleet Management CompanyDocument5 pagesOrg Structure Small Fleet Management CompanyIndresh Singh SalujaNo ratings yet
- Vehicle - Workshop Monitoring Template - V 1Document39 pagesVehicle - Workshop Monitoring Template - V 1Indresh Singh SalujaNo ratings yet
- Siva KumarDocument5 pagesSiva KumarIndresh Singh SalujaNo ratings yet
- Organisation Competitiveness IndexDocument8 pagesOrganisation Competitiveness IndexIndresh Singh SalujaNo ratings yet
- Organisation Competitiveness Index - IntroductionDocument3 pagesOrganisation Competitiveness Index - IntroductionIndresh Singh SalujaNo ratings yet
- Indresh Singh Saluja Profile 2014Document2 pagesIndresh Singh Saluja Profile 2014Indresh Singh SalujaNo ratings yet
- Preferably Male Candidate Essential Duties and ResponsibilitiesDocument1 pagePreferably Male Candidate Essential Duties and ResponsibilitiesIndresh Singh SalujaNo ratings yet
- MSB Tech Brochure 1Document4 pagesMSB Tech Brochure 1Indresh Singh SalujaNo ratings yet
- Organisation Competitiveness Index - IntroductionDocument3 pagesOrganisation Competitiveness Index - IntroductionIndresh Singh SalujaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- DATABASE Kawasan Industri PolugadungDocument20 pagesDATABASE Kawasan Industri PolugadungRina Rachman100% (1)
- 43 CSeT F Mock - 240818 PDFDocument26 pages43 CSeT F Mock - 240818 PDFben romdhane ahmedNo ratings yet
- 72-76 kW 310SK/310SK TC Compact Track Loader SpecsDocument10 pages72-76 kW 310SK/310SK TC Compact Track Loader SpecsPerrote Caruso PerritoNo ratings yet
- Ngos' Due Diligence and Risk Mitigation: A Holistic ApproachDocument54 pagesNgos' Due Diligence and Risk Mitigation: A Holistic ApproachMichel KozahNo ratings yet
- Occurrence of Black Soldier Fly HermetiaDocument2 pagesOccurrence of Black Soldier Fly HermetiaMarcelo Geraldo TeixeiraNo ratings yet
- Creativity & Innovation Notes - IV - Sem - 2016 PDFDocument31 pagesCreativity & Innovation Notes - IV - Sem - 2016 PDFPreityTripathi79% (14)
- Course 1 Introduction To SIMS: Student Information Management System (SIMS) Office of The RegistrarDocument28 pagesCourse 1 Introduction To SIMS: Student Information Management System (SIMS) Office of The RegistrarWeijia WangNo ratings yet
- Hydro Skimming Margins Vs Cracking MarginsDocument78 pagesHydro Skimming Margins Vs Cracking MarginsWon Jang100% (1)
- Cybersecurity Case 4Document1 pageCybersecurity Case 4Gaurav KumarNo ratings yet
- Biju Patnaik University of Technology MCA SyllabusDocument18 pagesBiju Patnaik University of Technology MCA SyllabusAshutosh MahapatraNo ratings yet
- Cambridge O Level: English Language 1123/21Document8 pagesCambridge O Level: English Language 1123/21Fred SaneNo ratings yet
- Form-Q - Application For Quarry PermitDocument1 pageForm-Q - Application For Quarry PermitDebasish PradhanNo ratings yet
- Panasonic Th-42pd50u Chassis Gp8duDocument147 pagesPanasonic Th-42pd50u Chassis Gp8du02ury05No ratings yet
- Safety Breach NoticeDocument3 pagesSafety Breach NoticeMohamed HadjkacemNo ratings yet
- Manual LubDocument25 pagesManual LubMota Guine InformaçõesNo ratings yet
- REXTAR User and Service GuideDocument58 pagesREXTAR User and Service GuidewellsuNo ratings yet
- New Form 2550 M Monthly VAT Return P 1 2 1Document3 pagesNew Form 2550 M Monthly VAT Return P 1 2 1The ApprenticeNo ratings yet
- 3 Human Resource ManagementDocument10 pages3 Human Resource ManagementRonaldNo ratings yet
- OBURE Understanding How Reits Market WorksDocument3 pagesOBURE Understanding How Reits Market WorksJohn evansNo ratings yet
- Catalogue: See Colour in A Whole New LightDocument17 pagesCatalogue: See Colour in A Whole New LightManuel AguilarNo ratings yet
- QRHDocument12 pagesQRHNwe OoNo ratings yet
- Display Kit GuideDocument9 pagesDisplay Kit GuidemfabianiNo ratings yet
- ASTMH Exam Brochure 18 FNLDocument17 pagesASTMH Exam Brochure 18 FNLNgô Khánh HuyềnNo ratings yet
- 2 C Program StructureDocument13 pages2 C Program StructurePargi anshuNo ratings yet
- Pizza Crust Menu in Karachi - Restaurant Online Ordering PakistanDocument2 pagesPizza Crust Menu in Karachi - Restaurant Online Ordering PakistanSyed Rafay HashmiNo ratings yet
- Appendix 27 - CASH RECEIPTS REGISTERDocument1 pageAppendix 27 - CASH RECEIPTS REGISTERPau PerezNo ratings yet
- Summer's TowerDocument8 pagesSummer's TowerSum SumNo ratings yet
- Rojo Session 3 Activity 2Document4 pagesRojo Session 3 Activity 2ESTHER ROSE ROJONo ratings yet
- Top 70 CCNA Interview QuestionsDocument10 pagesTop 70 CCNA Interview QuestionsRekha SharmaNo ratings yet
- BITUMINOUS MIX DESIGNDocument4 pagesBITUMINOUS MIX DESIGNSunil BoseNo ratings yet